It's been a while since I've found the time to write a blog post. I'm writing for Eli Lilly now, and you can check out some of those posts here ---> https://lillypad.lilly.com/?auth=76 I find a lot of the content I'm sharing over there to be stuff that I would also share on here, so no sense in duplicating!
We decorated for Christmas the day after Thanksgiving, marking the start of my most favorite holiday and time of the year. Christmas music is being piped throughout the house (and car and headphones) and reflections of the past year have inevitably begun. We had a tough go for the second half of this year, and we're sort of still in it. If you recall, Drew lost a significant amount of his lung function over the summer before we identified the culprit - a fungal infection. We treated him with anti-fungal medication and he thankfully improved until there was a second unexpected drop near the start of the school year. He had gotten back up to 91, and then in September dropped back down to 78. We had discussions about what might be causing it and what we should do to treat him, and decided to temporarily stay the course on the anti-fungal medication until he reaches and maintains a baseline on it, giving us confidence that it is both working and that the infection is under control. You may recall (or maybe not) that he had a fungal infection last year around this time. We started the anti-fungals for 3mo and he improved, so we stopped the treatment, and then by June he had lost 30% of his lung function, maybe not so mysteriously after all. I suggested that perhaps we hadn't had the infection under control as we had originally thought and, like fungus does, it slowly crept back wreaking silent havoc. I want to make sure that we are confident that things are under control this time before we change course, as a newer article suggests that fungus can become quite resistant if treated, if the medications used to treat it aren't used properly. The options seem to be, per this article anyway, treat the fungus and increase its adaptive skills, or not treat it and allow the pathogen to settle in the lungs. Not treating wasn't an option for us because of the impact that it was having on his lung function.
It's complicated, this disease. We seem to have the bacterial load in his lungs under control. Most research shows that bacterial exacerbations are a leading cause of lung function decline and lung damage in CF. But once we finally got the achromobacter under control with years of treatment on inhaled antibiotics and steroids, we seem to have traded it for a fungal infection. Did we cause the fungal infection? Perhaps we did, there's not really a good way to say. Is it better to have a bacterial infection or a fungal infection? I would probably argue that a fungal infection is *better* given that these is little research that shows the impact of a fungal infection on the progression of disease. I do not know if there is evidence to support the contrary, or just lack of research on this altogether. Either way, I'm interested to learn more and hope that the CFF will continue to study this.
He's got a cold now, coughing in his sleep and when he's running around and playing. We've added extra treatments which has him crankier than ever, but it's necessary. We've been going in to clinic for PFT's every two weeks and his numbers are remaining pretty consistent - 78, 81, 82 - but I'm not so sure how things will look with this new cold, perhaps something he picked up when we were in clinic for one of those appointments. Despite their best infection control practices - recently even declaring that the spread of infection among patients in our clinic had come to a halt with new infection control practices, which is great news - going into the hospital remains one of the most dangerous places for Drew to be. There are lots of sick people coming here for care, and even though we wear a mask and don't touch anything, he always seems to catch something when we have to come here. We should be able to use home spirometers to monitor our lung function. We should be able to track our weight from home, and other symptoms, and communicate what we learn with our care team, eliminating the need for unnecessary visits, saving everyone time and money, and perhaps even improving health. Machine learning can enable this, and should. While our center was using the Orchestra platform (which is no longer), we did start to see a longitudinal view of patients health shared with the care team. We did improve inter-visit communication, and intervention at more appropriate times rather than just when we happened to have a visit scheduled. It didn't reduce the number of times that we *needed* to come into clinic but it could have. I highlight the word *needed* as this is an evidence based medicine metric, a guideline put forth by the CFF for all patients, and embraced by all clinicians, regardless of whether its the right thing for the patient. The care teams aren't interested in reducing clinic visits below the required 4x a year. Or maybe they are interested but just can't becasue the CFF uses this as an accreditiation metric, requiring them to do this or find a way to improve rather than working to understand, from patients, why they aren't coming in 4x/yr and how we might work together to optimize care and outcomes according to the patient priorities. Hopefully our learning network will fix this. I digress.
I hope he's well for the holidays. I got this crazy idea to take my family to NYC to see some cousins the week before Christmas. What crazy person wouldn't want to drive 24hrs over 3 days to spend a night in a matchbox sized hotel room to see family and New York City at Christmastime?! I'm sure traffic will be delightful. At least we can stream Christmas music in the car!
I hope he feels well enough to open gifts with excitement and delight on Christmas morning, and that we don't have to pull him away from new toys to do extra treatments. I'd love to, for just one day, forget all of the medical stuff. I'd love to wake up and not have a schedule. I'd love to go out to dinner and not worry about hand sanitizer and enzymes. I'd love for him to run around outside, maybe in the snow, and not come back inside having a coughing fit, and rather than breathing treatments, have hot chocolate while all of the clothes defrost into a puddle in my foyer.
I've declined antibiotics for him since September because I don't think he needs them. Maybe I'm wrong, but I'm trusting my gut this time. We will go there if we need to, but for right now, we will do our treatment and take our medicine and listen to our Christmas music and enjoy this holiday as much as we can.
Wednesday, November 30, 2016
Sunday, November 13, 2016
Tuesday, November 8, 2016
Collaboration and Culture Change: The Valuable Role of Storytelling in Health Care Improvement
This post originally appeared on LillyPad, a blog for Eli Lilly Pharmaceuticals, where I write as an ePatient Advisor
Editors Note: Over the next few weeks we will spend some time listening to the stories of some ePatients who have been collaborating together on ways to show the value and importance of patients as partners, collaboration for improvement, and connection & learning through “the network” for healthcare improvement. It’s important that these stories be told beyond our Google Hangouts or private Facebook groups or dinner tables and pushed more deeply into prominent places in our society because you can’t have culture change without collaboration and you can’t collaborate on what you don’t know about.
There’s this weird feeling that happens after I return from a health conference. I’m so full of new ideas, having spent several days away focused only on the things I’m working on, being around only people who share my passions in this space. I get to put aside breathing treatments and medication ordering and insurance fighting as I listen to amazing presenters share about the phenomenal work they’re doing, trying to translate what they’re doing to what I do, always considering ways that we might be able to help one another. I eat lunch with unlikely partners and I’m fascinated by the wealth of knowledge they bring, wondering how on earth I got so lucky to have the opportunity to learn from them. Sometimes I’m the one presenting, proud of my work, anxious to share with others the ways that I believe what I do can also help them and their communities. Then there is dinner where we pack up “work” for a while and build relationships, getting to know one another on a more personal level – our interests, passions, families and friends. There’s a buzz that fills your soul and lifts your spirit.
Through these conversations, we realize a shared humanity and how our lives really are the fuel for the work that we do. When I hop on the plane to leave these meetings, I’m so full of energy and renewed hope. Then just like that, I am back to the rat race – preschool drop off, signing school folders, sporting events, field trips, breathing treatments and appointments and medications and worry. There’s a buzz at home too, but a very different buzz. I’m so grateful to be home to the hugs and the very important stories about who sat next to whom on the bus, trying to squeeze in dinner between homework and basketball practice, turning on a movie so that I can find five minutes of quiet to order the medication that we will run out of in three days. But no one here understands. Here, people are doing their jobs and living their lives. They didn’t get to experience what I just experienced, what changes me just a little bit every time it happens. And I realize that without this buzz at home I wouldn’t have the other.
There’s absolutely no question that I would trade everything to take cystic fibrosis (CF) away from my son and our family. There are days when I wish more than anything that I could go back to being “just a mom,” scheduling playdates and going on nature walks, not having to sit at home waiting to sign for this month’s medication delivery or change our plans due to an unplanned illness. Yes, CF is a horrible disease that just takes and takes. I cannot change the disease, but we can control how we respond to it.
CF has expanded my friend circle and my world view. I have such a deep appreciation for the experiences of others, and I often learn the most from the people I don’t agree with. This is what it means to be an advocate - loving so much that your heart could burst, and then channeling that love and balancing it against the fear of loss. There isn’t a right or wrong way to be an advocate, but it’s something that those of us in the trenches are uniquely qualified for. Everyone can stand up and tell their story in an empowering way, but sometimes diagnosis or disease progression pushes us closer to this. As we work in health care improvement as patient advocates, there’s a focus on data. But data, while it can persuade people, doesn’t always inspire them to act. To quote an amazing article on the power of storytelling, “To do that, you need to wrap your vision in a story that fires the imagination and stirs the soul.” This, I believe to be true.
I’m honored to be able to share my story with the world, one that challenges the paradigm for how you can work with patients and caregivers. Our lived experiences with research can help to grow our collective understanding of the benefits and challenges of participation – what is it that each of us want, and how can we collaborate to achieve that. Together, we can make the shift from reactive to proactive care. Together, we find answers and change outcomes.
The new musical Hamilton is a powerful story that celebrates our founding fathers, who launched a new era of government. I’d like to honor some of the “founding fathers” of a new era of patient partnership in health care. They have helped to create the foundation upon which this great community is being built. It is through our stories weaving the thread between us all that we will continue to learn and grow. Over the next few weeks, you will hear from advocates in both the diabetes and cancer communities sharing their stories related to the idea of patients as partners, collaboration for improvement, and connection and learning through “the network.” So, in the words of Lin-Manuel Miranda as Alexander Hamilton, “Let’s raise a glass to the four of us, tomorrow there’ll be more of us, telling the story of tonight.” We hope you enjoy our stories.
Monday, October 10, 2016
A Letter to the CF Learning Network
We all have the unique opportunity to see the world from a different vantage point. I, as the mother of a child with CF, first saw this community as one of fundraisers, patients and families with an endless hope for a cure, working tirelessly to make connections and fund research to cure this disease. The more I got to know these folks, I started to see teachers and fathers and technologists and marketers and musicians and policymakers. I got to know the care team that was helping me to care for my son, and I realized that they were also soccer moms and artists and advocates, quality improvement specialists who weren’t just caring for my son, but caring for my community. I got more involved and started to see through my work and social networks how many different groups were working on similar things – parent & patient groups, the CF Foundation, pharmaceutical companies, the government – yet all unaware of the work of the others, and I started to think about how we might help those people and that information to intersect so that more people could learn together and time could be saved.
And then I would get discouraged or frustrated – there are so many moving parts! How could I get the care center in City A to do what the care center in City B was doing that seemed to be addressing the specific issue they were having? How could I make sure that my son was getting the best, most personalized care for him, not just the best care that his care team knew about? How could I share access to all that I’ve learned so that others could benefit from it as well? I shouldn’t have to stumble upon information on Facebook at the right time to find benefit.
Sometimes we don’t know what we don’t know, but I think it’s safe to assume in 2016 that if you don’t know the answer to something, you can quickly figure out how to find it.
I see information being shared every moment of every day – doctors like Raouf sharing the success of implementation of the chronic care model and the work that he has done as the head of our pulmonary department to achieve this success; people like Emily Kramer Golingkoff starting her own research foundation with an urgency for progress because the trajectory of the science isn’t fast enough to save her life; folks like LaCrecia who understand the realities of CF centers of all shapes and sizes and the need for a standardized yet personalized approach to improvement after having served as a coach for many years. Everyone has something unique to offer, something complimentary to what the rest of us each bring. People like Jim Murphy with compassion and empathy that partner with families to understand their unique needs and work tirelessly to minimize the impact of the disease on our lives. Adrienne likes to read, cook, crochet, hike and travel the world in addition to the clinical expertise and experience she brings. Bruce’s leadership role enables him to help different groups both within and beyond the foundation to mingle for improvement and change. Breck is a fundraiser, a storyteller and an advocate, not only sharing what she knows but always eager to learn and connect. And folks like Tracey and Sophia and Sarah help us to stay on track, organizing our work and helping to create a roadmap out of the many pins we drop. Michael says yes. He encourages us to try new things, taking risks, and leads by doing. I bring and insatiable curiosity, a connection to a strong network of like-minded folks desperate for change, and a never-ending hope that people like Drew can be well, retaining the autonomy to make decisions in their life according to their own priorities, not according to cystic fibrosis.
People make connections in a network all the time. It’s not something we are advocating for. It is something that happens. I could go on and on about the strengths that we all have, but I suspect that as we part ways and reflect on the time we spent together we will all be well aware of the value of the contribution that each of us is making to this work.
There is a great TED Talk by a woman named Angela Blanchard that talks about how we, as a society, as people wanting to help, are trained to look at the problems - the lacks, gaps, needs, wants - the broken stuff, and how we can’t build on broken. She suggests that perhaps instead of looking at all that people don't have, we should start to look at what they do. I think this has a lot of relevance for this learning health system model we are moving toward. I can give you the example of an ENT appointment a few months ago. When we sat down in the office the nurse said, "So we have Andrew here, a 5yr old male with a history of cystic fibrosis, tracheomalacia, pancreatic insufficiency, more bronchoscopy's than I can count, chronic sinusitis, a bowel resection, ileostomy, and airway abnormalities. His medication list is about 4 pages long but I've gotta go through it so here we go." I interrupted her to say, "There’s a lot right with him, too." She chuckled and we moved on.
What if Angela Blanchard is exactly right and we can't build on broken. What if the answer lies in our ability as a team - patient and provider and researcher and foundation - to share what we have, and build what we can to find what we need. What if we can't see the solution by just looking at the problem? It is about partnership, but a different kind. A partnership focused on what we each have rather than what we each need.
The TED talk goes on to say “We've all been in situations, as humans, raw and painful and excruciating moments, and it's hard in those moments to think about asking people what they have, talking about their strengths, what they're good at.” But much like so many of us in this room feel compelled to help, in fact were trained to help, the patients/caregivers, we want to contribute too. All of our stories matter. We want to tell you what we can do and what we do know as that's the first step on my path to a new story. This gives us all hope, meaning, a sense of belonging. Think about how we might be able to shift away from the post-traumatic stress of diagnosis or disease progression and toward post traumatic resilience, something that science has proven comes when one feels they are making a meaningful contribution. Think about how that might translate to successful transitions, adherence, sustainability, success. We all have the capacity to imagine a future different from the life we live. The job of those who want to help , those of us in this room today, is to stand together.
I believe that success of our work will be dependent upon this enhanced appreciation of what we each have. I encourage you to listen to one another, like really listen, especially when you don’t agree or you hear something unexpected, for its these moments that we can most learn from. Its something I’ve been working on and its paid off big time.
My wish for the CF Community is that we can work together to figure out how to pull our strengths together to create something better than any of us can create alone, laying the tracks for the greater CF community to see the potential in themselves and contribute to create change.
We’ve had an incredibly impressive group of folks in this room for the past two days, from White House Champions of Change to esteemed scholars, members of PCORI and the Institute for Healthcare Improvement and people with CF and parents who find the time to step away from the demands of this disease to help. And that’s just whose in this room. When you think about the CF Community more broadly and consider all that they have and all that they do, there is no doubt that we will succeed in our work. Thanks for being here and for the unique gifts that you bring. Let’s do this!!!
And then I would get discouraged or frustrated – there are so many moving parts! How could I get the care center in City A to do what the care center in City B was doing that seemed to be addressing the specific issue they were having? How could I make sure that my son was getting the best, most personalized care for him, not just the best care that his care team knew about? How could I share access to all that I’ve learned so that others could benefit from it as well? I shouldn’t have to stumble upon information on Facebook at the right time to find benefit.
Sometimes we don’t know what we don’t know, but I think it’s safe to assume in 2016 that if you don’t know the answer to something, you can quickly figure out how to find it.
I see information being shared every moment of every day – doctors like Raouf sharing the success of implementation of the chronic care model and the work that he has done as the head of our pulmonary department to achieve this success; people like Emily Kramer Golingkoff starting her own research foundation with an urgency for progress because the trajectory of the science isn’t fast enough to save her life; folks like LaCrecia who understand the realities of CF centers of all shapes and sizes and the need for a standardized yet personalized approach to improvement after having served as a coach for many years. Everyone has something unique to offer, something complimentary to what the rest of us each bring. People like Jim Murphy with compassion and empathy that partner with families to understand their unique needs and work tirelessly to minimize the impact of the disease on our lives. Adrienne likes to read, cook, crochet, hike and travel the world in addition to the clinical expertise and experience she brings. Bruce’s leadership role enables him to help different groups both within and beyond the foundation to mingle for improvement and change. Breck is a fundraiser, a storyteller and an advocate, not only sharing what she knows but always eager to learn and connect. And folks like Tracey and Sophia and Sarah help us to stay on track, organizing our work and helping to create a roadmap out of the many pins we drop. Michael says yes. He encourages us to try new things, taking risks, and leads by doing. I bring and insatiable curiosity, a connection to a strong network of like-minded folks desperate for change, and a never-ending hope that people like Drew can be well, retaining the autonomy to make decisions in their life according to their own priorities, not according to cystic fibrosis.
People make connections in a network all the time. It’s not something we are advocating for. It is something that happens. I could go on and on about the strengths that we all have, but I suspect that as we part ways and reflect on the time we spent together we will all be well aware of the value of the contribution that each of us is making to this work.
There is a great TED Talk by a woman named Angela Blanchard that talks about how we, as a society, as people wanting to help, are trained to look at the problems - the lacks, gaps, needs, wants - the broken stuff, and how we can’t build on broken. She suggests that perhaps instead of looking at all that people don't have, we should start to look at what they do. I think this has a lot of relevance for this learning health system model we are moving toward. I can give you the example of an ENT appointment a few months ago. When we sat down in the office the nurse said, "So we have Andrew here, a 5yr old male with a history of cystic fibrosis, tracheomalacia, pancreatic insufficiency, more bronchoscopy's than I can count, chronic sinusitis, a bowel resection, ileostomy, and airway abnormalities. His medication list is about 4 pages long but I've gotta go through it so here we go." I interrupted her to say, "There’s a lot right with him, too." She chuckled and we moved on.
What if Angela Blanchard is exactly right and we can't build on broken. What if the answer lies in our ability as a team - patient and provider and researcher and foundation - to share what we have, and build what we can to find what we need. What if we can't see the solution by just looking at the problem? It is about partnership, but a different kind. A partnership focused on what we each have rather than what we each need.
The TED talk goes on to say “We've all been in situations, as humans, raw and painful and excruciating moments, and it's hard in those moments to think about asking people what they have, talking about their strengths, what they're good at.” But much like so many of us in this room feel compelled to help, in fact were trained to help, the patients/caregivers, we want to contribute too. All of our stories matter. We want to tell you what we can do and what we do know as that's the first step on my path to a new story. This gives us all hope, meaning, a sense of belonging. Think about how we might be able to shift away from the post-traumatic stress of diagnosis or disease progression and toward post traumatic resilience, something that science has proven comes when one feels they are making a meaningful contribution. Think about how that might translate to successful transitions, adherence, sustainability, success. We all have the capacity to imagine a future different from the life we live. The job of those who want to help , those of us in this room today, is to stand together.
I believe that success of our work will be dependent upon this enhanced appreciation of what we each have. I encourage you to listen to one another, like really listen, especially when you don’t agree or you hear something unexpected, for its these moments that we can most learn from. Its something I’ve been working on and its paid off big time.
My wish for the CF Community is that we can work together to figure out how to pull our strengths together to create something better than any of us can create alone, laying the tracks for the greater CF community to see the potential in themselves and contribute to create change.
We’ve had an incredibly impressive group of folks in this room for the past two days, from White House Champions of Change to esteemed scholars, members of PCORI and the Institute for Healthcare Improvement and people with CF and parents who find the time to step away from the demands of this disease to help. And that’s just whose in this room. When you think about the CF Community more broadly and consider all that they have and all that they do, there is no doubt that we will succeed in our work. Thanks for being here and for the unique gifts that you bring. Let’s do this!!!
Sunday, September 25, 2016
Let's talk about evidence
"We don't seek the painful experiences that hue our identity, but we seek our identity in the wake of painful experiences."
I don't know where this quote came from, only that I find so much truth in it. If whoever wrote it happens to read this, raise your hand so I can learn more from you.
Cystic Fibrosis sucks so bad. You can't usually see it, yet it forces you to act - restraining your kid for necessary blood work to make sure the medication we're taking to save his lungs isn't killing his liver. Childhood playtime after school is stolen from us as we sit for hours doing breathing treatments and airway clearance instead of going to the park without an agenda. A hug allows me to literally feel a mucus plug trapped deep in his airways, something I can loosen with a few aggressive beats on his chest and I do it without warning as he would deny my offer to help because of the pain it causes him while simultaneously offering some relief. And I sit on an airplane on my way to my second conference in two weeks, having received great news in the 4 days I was home, and yet I cry because I know that the relief I feel is temporary. Hopefully optimistic but not naive. Despite our best efforts this disease will progress. I can sit by the pool at my favorite hotel in Palo Alto so incredibly grateful for these people I've met because of this disease, and cry as I walk back to my room moments later cursing the world and wishing it all away in a trade for normalcy. I don't know normalcy though, I suppose. This is our normal. It's breathtaking to see the world in this way, a gift not many people get. And I love it and hate it equal parts.
Drew's lung function tanked this summer. We saw his doctors many times, and I used my personal network to crowd source ideas for what might be wrong. Early on, there were suggestions by my peers that a fungal infection might be the culprit. With no symptoms except for a rapidly declining FEV1, we spent countless hours troubleshooting - trying everything in our "evidence-based" bag of tricks. There's not significant evidence to suggest that fungus causes lung function decline in people with CF. Or I guess I should say that there's not peer-reviewed published scientific evidence. The "evidence" that I have, the experiences of the people living with cystic fibrosis who have lived through our same uncertain hell, is often discounted. And I get it, really. I am pro evidence-based medicine. I just can't help but think about the value of the individual human experience we are missing.
Despite there being no physical symptoms of exacerbation - data that I have based on our prior experiences, things that are in fact documented in his EHR - we opted for treating this like an exacerbation because we didn't know what else to do. The "we" I speak of is us and his care team. The first step was an oral antibiotic. Drew has never responded to oral antibiotics. I was skeptical of this plan but ultimately on board. After 10 days, there was actually increased decline. He has found benefit from steroids in the past due to the wonky nature of his airways, but I can identify with accuracy the situations that will be improved with steroids and this wasn't one of them. We tried anyway. The downside was outrageous mood swings. While medically induced, I still expect certain behaviors from my kids, and its absolutely heartbreaking to watch your 6yo, who feels like he's going to jump out of his skin and not understand why, sob in his bedroom for hours because, medication or not, hitting other people is not ok. The steroid may have slowed the decline, but his lung function continued to drop.
When we have to make the hard decisions about whether or not to try IV antibiotics, more frustration and disappointment came out of fear, from all of us, that yet another treatment, another procedure would render the same results and we would be left with even fewer options. It's so hard to balance these decisions. His health is a priority, but so is his life, and living means so much more than being alive. Can I take away the joy of the pool or the promised vacation with the hope that this could put us back on track? How could I convince him that this is the right thing to do when all of the preventative medicine he takes, the stuff we tell him we must do for hours every day to keep him healthy has left him so very sick. What the fuck kind of sick logic does this disease demand?
We opt for a combination of IV medications that we hope would target the bacteria that we suspect might be causing the problem, weighing dosing schedules against our ability to administer them from home because there's no way we are admitting him to the hospital when he looks and feels fine. We trade sleep for this decision and our whole world pays for it. Work commitments change and home routines suffer as patience wears thin. Tired and terrified while pretending to be neither is a bad combination. And yet we continue, a constant barrage of choices in our faces, very serious ones with real consequences.
They told us when he had his PICC placed that we might want to have a conversation with our team about a port given the increasing difficulty with placement of a central line due to the fact that he's had 9 in his 6 years of life and scar tissue is getting in the way. With some ativan to take the edge off, we both cried as they stuck him, then stuck him again. His fear has scars showing the distance he's come. I have fear too, but all of my scars are on the inside. I'm a little tougher to break, and each time we do this feels a little more routine, a little more scary.
The IV meds didn't help either. With our lung function creeping closer and closer to 70%, we re-group for another team meeting. I want to know all of the options. We decide on a bronchoscopy, something that will allow them to get a reasonable sample of what might be in his lungs and enable us to target our therapy. Why didn't we start here? Everything comes with its own risks, and the care team was hopeful that we could address the problem more easily. I trust them and agreed with their plan. I also asked about the risks of treating with an anti-fungal medication. After all, we just followed the script for oral and IV antibiotics and also a steroid, each with its own risks, especially given that they seemed to be the wrong choice as they showed no clinical benefit and the risks of antibiotic resistance in this population is enormous. There is not evidence to support a fungal infection causing a decline in lung function, or "published, peer-reviewed, scientific evidence" anyway. There is a surplus of anecdotal experiential evidence.
With a family vacation just a day away, we go to the hospital for this outpatient procedure. I do my best distraction song and dance while they give him sleepy air. My husband and I don't even go to these together anymore because we've been through them so many times, and life and work don't pause for this disease. I anxiously wait to be called back to see the doctor in what I can only describe to be the purgatory that is the same day surgery waiting room. Her words have so much power to change my life and I'm terrified. But all looks good! His lungs look as good on the inside as they sounds on the outside and we are left wondering. We have to wait 5 long days to see what grows on the culture, to see what explanation we might get from another piece of data. I've convinced that I lose about a day of my life in this unavoidable worry that comes from this unavoidable waiting.
By now, his doctor has given me a prescription for the anti-fungal medication I've been asking for. I promised not to use it until after the bronch, We agree that we have nothing to lose by starting it while we go on our vacation and wait for our results. When the results do come back and show that he has a fungal infection, we exchange emails with his care team about their lack of optimism that the anti-fungal will have an impact given the type of fungus he has, a more common household name I'm told, but without other options it seems to be the last resort and we go forward.
After 4 weeks on the treatment, we wake up early, get our treatments done before the sun comes up, and head into the office for an assessment. I have a preference for the 7:30am Monday morning appointment as I believe it lowers the cross-infection risk, something that no evidence exists for. It gives me some resolve to have this time slot and I'm grateful to the team that recognizes that and works to accommodate me. He's up to 84! It seems to be working! He's re-gained more 10pts of that lost lung functions and we are elated! We decide to stay the course and after another 4 weeks he is up to 91. I express my joy to his care team who is equally delighted, admitting their early skepticism about this being the cause of the problem and acknowledging the treatment as the reason for our success. I certainly didn't set out to prove anyone wrong, only to make him well, but it's nice to hear that they are learning along with me.
This is a happy story, but it's not the end of the story. We will have treatment decisions to make again next month - stay the course? Make a change? What changes will happen that will be out of our control? Will the next culture show a bug that's completely resistant? Is there anything I can do to prevent that? To protect him?
The past two courses of IV antibiotics that Drew has had have not been needed. We treated a bad case of acid reflux and a fungal infection with hard core antibiotics. We followed the guidelines and used decision trees and made the decisions that we felt we had to make, and we were wrong. Drew has been on inhaled antibiotics - 2 different medications alternated in 15 day cycles, inhaled 3x a day, everyday for the past 3 years. In those 3 years he has not had a bacterial infection in his lungs, an "exacerbation". In 3 years he has not gotten sick. He's been on IV and oral antibiotics that he hasn't needed, and been sedated countless times. He has been admitted for central line infections for central lines he hasn't needed, all because we followed the rules. I don't think we made a mistake, we did what we knew how to do. But now that we know better we need to do better. I wholeheartedly believe there has to be a better way. We might talk about the risks of exploring medications or procedures that lack "evidence", but I also want to talk about the risks of evidence based medications and treatments that we use when we don't need them. How might we get the right thing to the right person at the right time, every time? How might we improve the mental health of our patients and caregivers who are rightfully distraught over the lack of answers to what should be straightforward questions? Why is there still so much uncertainty in medicine? What responsibility should we put on people to advocate for themselves, tracking their own outcomes and then sharing them with the rest of the healthcare system to enable personalization of treatments, and then machine learning to aggregate all of these N of 1's, improving population health through the spread of personalized solutions.
Some new opportunities have recently come my way to improve things within the healthcare system. My goals remain the same - right person, right solution, right time, every time. I think success is more than just improved outcomes just as living is more than just being alive. Success for me is influence. When more people believe that this is possible, when they challenge the status quo and try out of the box solutions, that feels like success. I know I'm making a difference. We are farther in this culture change than we were 5 years ago when I realized my purpose in all of this. As I fly to another healthcare conference, my second in two weeks - a conference where patients and caregivers are being introduced to the world as a symbol of action and influence, a conference where our participation is being fully financially supported - I know that my role is to honestly and vulnerably share these stories and ideas for change. I've figured out how to fold the worst narrative of my life into triumph, and that for me is how I measure success.
I don't know where this quote came from, only that I find so much truth in it. If whoever wrote it happens to read this, raise your hand so I can learn more from you.
Cystic Fibrosis sucks so bad. You can't usually see it, yet it forces you to act - restraining your kid for necessary blood work to make sure the medication we're taking to save his lungs isn't killing his liver. Childhood playtime after school is stolen from us as we sit for hours doing breathing treatments and airway clearance instead of going to the park without an agenda. A hug allows me to literally feel a mucus plug trapped deep in his airways, something I can loosen with a few aggressive beats on his chest and I do it without warning as he would deny my offer to help because of the pain it causes him while simultaneously offering some relief. And I sit on an airplane on my way to my second conference in two weeks, having received great news in the 4 days I was home, and yet I cry because I know that the relief I feel is temporary. Hopefully optimistic but not naive. Despite our best efforts this disease will progress. I can sit by the pool at my favorite hotel in Palo Alto so incredibly grateful for these people I've met because of this disease, and cry as I walk back to my room moments later cursing the world and wishing it all away in a trade for normalcy. I don't know normalcy though, I suppose. This is our normal. It's breathtaking to see the world in this way, a gift not many people get. And I love it and hate it equal parts.
Drew's lung function tanked this summer. We saw his doctors many times, and I used my personal network to crowd source ideas for what might be wrong. Early on, there were suggestions by my peers that a fungal infection might be the culprit. With no symptoms except for a rapidly declining FEV1, we spent countless hours troubleshooting - trying everything in our "evidence-based" bag of tricks. There's not significant evidence to suggest that fungus causes lung function decline in people with CF. Or I guess I should say that there's not peer-reviewed published scientific evidence. The "evidence" that I have, the experiences of the people living with cystic fibrosis who have lived through our same uncertain hell, is often discounted. And I get it, really. I am pro evidence-based medicine. I just can't help but think about the value of the individual human experience we are missing.
Despite there being no physical symptoms of exacerbation - data that I have based on our prior experiences, things that are in fact documented in his EHR - we opted for treating this like an exacerbation because we didn't know what else to do. The "we" I speak of is us and his care team. The first step was an oral antibiotic. Drew has never responded to oral antibiotics. I was skeptical of this plan but ultimately on board. After 10 days, there was actually increased decline. He has found benefit from steroids in the past due to the wonky nature of his airways, but I can identify with accuracy the situations that will be improved with steroids and this wasn't one of them. We tried anyway. The downside was outrageous mood swings. While medically induced, I still expect certain behaviors from my kids, and its absolutely heartbreaking to watch your 6yo, who feels like he's going to jump out of his skin and not understand why, sob in his bedroom for hours because, medication or not, hitting other people is not ok. The steroid may have slowed the decline, but his lung function continued to drop.
When we have to make the hard decisions about whether or not to try IV antibiotics, more frustration and disappointment came out of fear, from all of us, that yet another treatment, another procedure would render the same results and we would be left with even fewer options. It's so hard to balance these decisions. His health is a priority, but so is his life, and living means so much more than being alive. Can I take away the joy of the pool or the promised vacation with the hope that this could put us back on track? How could I convince him that this is the right thing to do when all of the preventative medicine he takes, the stuff we tell him we must do for hours every day to keep him healthy has left him so very sick. What the fuck kind of sick logic does this disease demand?
We opt for a combination of IV medications that we hope would target the bacteria that we suspect might be causing the problem, weighing dosing schedules against our ability to administer them from home because there's no way we are admitting him to the hospital when he looks and feels fine. We trade sleep for this decision and our whole world pays for it. Work commitments change and home routines suffer as patience wears thin. Tired and terrified while pretending to be neither is a bad combination. And yet we continue, a constant barrage of choices in our faces, very serious ones with real consequences.
They told us when he had his PICC placed that we might want to have a conversation with our team about a port given the increasing difficulty with placement of a central line due to the fact that he's had 9 in his 6 years of life and scar tissue is getting in the way. With some ativan to take the edge off, we both cried as they stuck him, then stuck him again. His fear has scars showing the distance he's come. I have fear too, but all of my scars are on the inside. I'm a little tougher to break, and each time we do this feels a little more routine, a little more scary.
The IV meds didn't help either. With our lung function creeping closer and closer to 70%, we re-group for another team meeting. I want to know all of the options. We decide on a bronchoscopy, something that will allow them to get a reasonable sample of what might be in his lungs and enable us to target our therapy. Why didn't we start here? Everything comes with its own risks, and the care team was hopeful that we could address the problem more easily. I trust them and agreed with their plan. I also asked about the risks of treating with an anti-fungal medication. After all, we just followed the script for oral and IV antibiotics and also a steroid, each with its own risks, especially given that they seemed to be the wrong choice as they showed no clinical benefit and the risks of antibiotic resistance in this population is enormous. There is not evidence to support a fungal infection causing a decline in lung function, or "published, peer-reviewed, scientific evidence" anyway. There is a surplus of anecdotal experiential evidence.
With a family vacation just a day away, we go to the hospital for this outpatient procedure. I do my best distraction song and dance while they give him sleepy air. My husband and I don't even go to these together anymore because we've been through them so many times, and life and work don't pause for this disease. I anxiously wait to be called back to see the doctor in what I can only describe to be the purgatory that is the same day surgery waiting room. Her words have so much power to change my life and I'm terrified. But all looks good! His lungs look as good on the inside as they sounds on the outside and we are left wondering. We have to wait 5 long days to see what grows on the culture, to see what explanation we might get from another piece of data. I've convinced that I lose about a day of my life in this unavoidable worry that comes from this unavoidable waiting.
By now, his doctor has given me a prescription for the anti-fungal medication I've been asking for. I promised not to use it until after the bronch, We agree that we have nothing to lose by starting it while we go on our vacation and wait for our results. When the results do come back and show that he has a fungal infection, we exchange emails with his care team about their lack of optimism that the anti-fungal will have an impact given the type of fungus he has, a more common household name I'm told, but without other options it seems to be the last resort and we go forward.
After 4 weeks on the treatment, we wake up early, get our treatments done before the sun comes up, and head into the office for an assessment. I have a preference for the 7:30am Monday morning appointment as I believe it lowers the cross-infection risk, something that no evidence exists for. It gives me some resolve to have this time slot and I'm grateful to the team that recognizes that and works to accommodate me. He's up to 84! It seems to be working! He's re-gained more 10pts of that lost lung functions and we are elated! We decide to stay the course and after another 4 weeks he is up to 91. I express my joy to his care team who is equally delighted, admitting their early skepticism about this being the cause of the problem and acknowledging the treatment as the reason for our success. I certainly didn't set out to prove anyone wrong, only to make him well, but it's nice to hear that they are learning along with me.
This is a happy story, but it's not the end of the story. We will have treatment decisions to make again next month - stay the course? Make a change? What changes will happen that will be out of our control? Will the next culture show a bug that's completely resistant? Is there anything I can do to prevent that? To protect him?
The past two courses of IV antibiotics that Drew has had have not been needed. We treated a bad case of acid reflux and a fungal infection with hard core antibiotics. We followed the guidelines and used decision trees and made the decisions that we felt we had to make, and we were wrong. Drew has been on inhaled antibiotics - 2 different medications alternated in 15 day cycles, inhaled 3x a day, everyday for the past 3 years. In those 3 years he has not had a bacterial infection in his lungs, an "exacerbation". In 3 years he has not gotten sick. He's been on IV and oral antibiotics that he hasn't needed, and been sedated countless times. He has been admitted for central line infections for central lines he hasn't needed, all because we followed the rules. I don't think we made a mistake, we did what we knew how to do. But now that we know better we need to do better. I wholeheartedly believe there has to be a better way. We might talk about the risks of exploring medications or procedures that lack "evidence", but I also want to talk about the risks of evidence based medications and treatments that we use when we don't need them. How might we get the right thing to the right person at the right time, every time? How might we improve the mental health of our patients and caregivers who are rightfully distraught over the lack of answers to what should be straightforward questions? Why is there still so much uncertainty in medicine? What responsibility should we put on people to advocate for themselves, tracking their own outcomes and then sharing them with the rest of the healthcare system to enable personalization of treatments, and then machine learning to aggregate all of these N of 1's, improving population health through the spread of personalized solutions.
Some new opportunities have recently come my way to improve things within the healthcare system. My goals remain the same - right person, right solution, right time, every time. I think success is more than just improved outcomes just as living is more than just being alive. Success for me is influence. When more people believe that this is possible, when they challenge the status quo and try out of the box solutions, that feels like success. I know I'm making a difference. We are farther in this culture change than we were 5 years ago when I realized my purpose in all of this. As I fly to another healthcare conference, my second in two weeks - a conference where patients and caregivers are being introduced to the world as a symbol of action and influence, a conference where our participation is being fully financially supported - I know that my role is to honestly and vulnerably share these stories and ideas for change. I've figured out how to fold the worst narrative of my life into triumph, and that for me is how I measure success.
Thursday, September 8, 2016
Patients Included. But are we respected?
This post originally appeared on my blog in October of 2013.
"Any man or institution that tries to rob me of my dignity will lose because I will not part with it at any price or under any pressure." - Nelson Mandela, Long Walk to Freedom
A few weeks ago, I was asked to be a part of a Cystic Fibrosis work group at a hospital on the east coast under a grant from the Patient Centered Outcomes Research institute, or PCORI. A colleague had recommended me for the position, knowing my passion for collaborative efforts in improving outcomes and the value of the patient voice in research. Below is an excerpt from the email that I received:
PCORI was founded under the ACA to fund comparative effectiveness research that improves the information available to patients in a meaningful way. Specifically, PCORI has two goals: further engage patients in research design, and reduce the gap between research results and patient knowledge. The CDRN opportunity grants institutions money to develop a large multi-million patient data warehouse for researchers (from around the country) to conduct research - both prospectively and retrospectively. PCORI will fund seven of these networks around the country to form one national network. If awarded the grant, our team would like to offer you a role as a Cystic Fibrosis Community Workgroup member.
My interest peaked, I wrote back and a day later had an interview and was submitting my biosketch and a letter of support. I made them aware of the other work I'm currently involved with to ensure there would be no conflict of interest, and expressed the need to weigh the time commitment and opportunity for compensation with these other projects. Then, as if to define how they value my knowledge, experience, and expertise, I received this reply:
While this particular position will likely be unpaid, this is an incredible opportunity to directly influence the research efforts around CF and will provide you with access to cutting edge researchers in our city.
Is my time and participation not valuable enough to compensate?
Later that week, I packed my bags and headed to MedicineX in Stanford, California, a conference that positions itself as a catalyst for new ideas about the future of medicine and emerging technologies. At this conference, there were patients and clinicians, caregivers and technologists, entrepreneurs and researchers and others from the industry. It’s difficult to explain the experience of being at a conference so full of energy, excitement and hope for better care of rare diseases and chronic conditions, better interactions with the healthcare system, and how the only way to improve is collaboration and teamwork, valuing and trusting one another, in every single possible way.
During the first day of this conference, PCORI -- the organization offering the grant mentioned above -- was presenting a panel on the importance of involving patients in research. I wondered about the offer I had received: Was it the institution that could not offer to compensate me for my time? Or PCORI that isn't accommodating patients who participate in the research by appropriately and fairly compensating them? Or maybe just not all patients? Some view the amount that I work to improve health and care in Cystic Fibrosis as remarkable. I view it as necessary. If I had endless capacity, I would do it all. But remember, I have a seriously and chronically ill child that I am caring for, in addition to 3 others, and a husband, and a couple of fish. Unlike many researchers, I don’t have an institution or grants paying me a full time salary to participate in such research.
My reaction: Don't take advantage of the knowledge and experience that I have that you want and need to create a system that works for me. Appreciate me, and embrace me just as you would any other member of your team, and just watch how far we can go together.
A huge barrier to true patient-centered care is the failure to see patients as equals to the other contributors in this system. Let's not forget than in medicine, the patient is the only one who is expert in her experience. Should the hospital that offered me the position in their workgroup receive the grant from PCORI at the end of the year, I will participate and my participation will not be in vain. I said yes, regardless of compensation status, because I know and appreciate the value of this project. I have a unique perspective to bring that I believe will add value to this research and benefit others in the community. I said yes, because so many other people who have expertise and passion and value to add don't have the time or the voice or the energy to do it. I believe that our story, in the end, will be one of success. But to quote an incredible patient and advocate that I had the great pleasure to meet in person this weekend, "Not every medicine story can have a happy ending. It's not the ending that makes it a success."
How much farther and faster could this patient-centered research go if it weren't so hard to be a part of it?
Saturday, August 6, 2016
Research is Hope
“Hope” is the thing with feathers -
That perches in the soul -
And sings the tune without the words -
And never stops - at all"
I had to give my baby to strangers when he was two days old, signing papers to waive liability if something happened to him when he was under the care of someone I had never even met. This is the story of most chronic illness caregivers. As time goes on, our comfort level grows, relationships build with our doctors and care teams. But with chronic illness, or CF, anyway, in our case, there is always something new, always something scary, always something we don't understand. Then researchers come in - knocking on the door after a long 3 hr appointment, or while we are in the surgery holding area waiting to go back and wondering how the results of whatever we're having done will forever change our reality, yet holding it together for our kid who is equally scared - trying to explain what the researcher whose interested in a sample of our tissue or some of our thoughts (neither of which we're giving with a clear mind) is trying to do, what they're hoping to learn. But in that instant it sounds promising so we go with it, signing their paper since the risks seem low, collecting our gift card for participation, or just their thanks, in many cases, and the promise of learning or better connection with our care team, whatever it is that their trying to do. Hope is really what their offering us, and we sign up.
Sometimes there's further interaction, but many times not. Then months later, long after we've signed their papers, something hits us and we remember that time we signed up for that thing, and a bit of us wonders what ever came of it. And, if we search just a little bit, we find out that the study didn't recruit, or that it didn't meet the appropriate end points, or that the institution supporting it didn't see the value in it and it's done. Those researchers move on to their next theory to test and our contribution has been tossed aside. Or maybe it went on and that researcher learned many great things that they wrote about and got credit for and published their findings in some fancy journal that we don't have access to because, after all, we're just the patient. Forget about what the patient thought, what they learned, that brief glimmer of hope.
It feels abusive, really, to approach the sick and offer them hope - to take something from them, physical or otherwise, something that's so sacred - and then to just end it because it didn't meet your goals. When do my goals matter?
Why are we allowed to just throw that all away? Why is that ok? Shouldn't there be, if nothing else, a moral or ethical obligation to say, "I'm sorry, I tried." Shouldn't we be giving patients the opportunity to take what's been learned from the work they contributed to - the work that couldn't have been done without them - and start from a new baseline of learning? Why aren't we sharing what we are learning in research, successful or failed, in a way that allows folks to build upon it? This is among the greatest failures of modern medicine.
I want to ask researchers what they're actually trying to do. If the answer isn't that you are trying to, wholeheartedly, help patients, then please stop wasting our time.
A research project I had been a part of recently shut down and I'm so...I guess sad is the right word. I wasn't a participant, but rather a member of the study team so I can't help but feel a bit of responsibility. My frustrations are for those families who joined this project, sharing with us their precious time, the intimate details of their health and lives. People who were given hope only to be shown another dead end, and for no good reason. My participation and contributions felt uncomfortable at times. It was frustrating to have my ideas and suggestions for a more patient-centric approach limited by both institutional research regulations, and the discomfort or fear or I'm not exactly sure what of trying to do something different than it had ever been done previously. I should have pushed harder.
Helping patients means doing things differently than they're being done right now. I do believe researchers are trying to learn, to help us. But to be honest, it's moving at a devastatingly slow pace and it's too often letting us down.
Give me back what you've taken from me and encourage me to share it, to build upon it, to figure out what else we can learn together. My participation in research and the view I have of the participation of my peers has left me feeling exposed and uncomfortable, not wanting to say yes to future engagement. This is a problem that we need to fix! This is how we will really start to learn and grow and change and improve. Stop picking on the weaker man.
Research is Hope
“Hope” is the thing with feathers -
That perches in the soul -
And sings the tune without the words -
And never stops - at all"
I had to give my baby to strangers when he was two days old, signing papers to waive liability if something happened to him when he was under the care of someone I had never even met. This is the story of most chronic illness caregivers. As time goes on, our comfort level grows, relationships build with our doctors and care teams. But with chronic illness, or CF, anyway, in our case, there is always something new, always something scary, always something we don't understand. Then researchers come in - knocking on the door after a long 3 hr appointment, or while we are in the surgery holding area waiting to go back and wondering how the results of whatever we're having done will forever change our reality, yet holding it together for our kid who is equally scared - trying to explain what the researcher whose interested in a sample of our tissue or some of our thoughts (neither of which we're giving with a clear mind) is trying to do, what they're hoping to learn. But in that instant it sounds promising so we go with it, signing their paper since the risks seem low, collecting our gift card for participation, or just their thanks, in many cases, and the promise of learning or better connection with our care team, whatever it is that their trying to do. Hope is really what their offering us, and we sign up.
Sometimes there's further interaction, but many times not. Then months later, long after we've signed their papers, something hits us and we remember that time we signed up for that thing, and a bit of us wonders what ever came of it. And, if we search just a little bit, we find out that the study didn't recruit, or that it didn't meet the appropriate end points, or that the institution supporting it didn't see the value in it and it's done. Those researchers move on to their next theory to test and our contribution has been tossed aside. Or maybe it went on and that researcher learned many great things that they wrote about and got credit for and published their findings in some fancy journal that we don't have access to because, after all, we're just the patient. Forget about what the patient thought, what they learned, that brief glimmer of hope.
It feels abusive, really, to approach the sick and offer them hope - to take something from them, physical or otherwise, something that's so sacred - and then to just end it because it didn't meet your goals. When do my goals matter?
Why are we allowed to just throw that all away? Why is that ok? Shouldn't there be, if nothing else, a moral or ethical obligation to say, "I'm sorry, I tried." Shouldn't we be giving patients the opportunity to take what's been learned from the work they contributed to - the work that couldn't have been done without them - and start from a new baseline of learning? Why aren't we sharing what we are learning in research, successful or failed, in a way that allows folks to build upon it? This is among the greatest failures of modern medicine.
I want to ask researchers what they're actually trying to do. If the answer isn't that you are trying to, wholeheartedly, help patients, then please stop wasting our time.
A research project I had been a part of recently shut down and I'm so...I guess sad is the right word. I wasn't a participant, but rather a member of the study team so I can't help but feel a bit of responsibility. My frustrations are for those families who joined this project, sharing with us their precious time, the intimate details of their health and lives. People who were given hope only to be shown another dead end, and for no good reason. My participation and contributions felt uncomfortable at times. It was frustrating to have my ideas and suggestions for a more patient-centric approach limited by both institutional research regulations, and the discomfort or fear or I'm not exactly sure what of trying to do something different than it had ever been done previously. I should have pushed harder.
Helping patients means doing things differently than they're being done right now. I do believe researchers are trying to learn, to help us. But to be honest, it's moving at a devastatingly slow pace and it's too often letting us down.
Give me back what you've taken from me and encourage me to share it, to build upon it, to figure out what else we can learn together. My participation in research and the view I have of the participation of my peers has left me feeling exposed and uncomfortable, not wanting to say yes to future engagement. This is a problem that we need to fix! This is how we will really start to learn and grow and change and improve. Stop picking on the weaker man.
Friday, July 29, 2016
Vacation FTW!
This vacation.... You guys, this vacation was the most vacation-y vacation I think I've ever been on. Yes, the kids were there, and yes it was hotter than just about anywhere we've ever been, but the "wake up when you want" and the "walk to the beach in 5" and the "getting in the pool a moment after someone's says 'Hey does anyone wanna go in the pool'"....and it being 85ish in there when you jump in. And I haven't even mentioned the shrimp and grits yet, or the oysters and fried chicken. A day at the spa and having someone rub my feet for an hour. RUB MY FEET FOR AN HOUR!! We're doing puzzles and playing euchre, coloring and crafting and moving at a pace that everyone should try. Clear minds here. There's not a schedule. If you wanna go sightseeing you just do it. And if you wanna go out for breakfast you just go. There's no "we need to get home for..." and there's no answering emails or solving problems because there aren't any problems. I'm reading a book instead of a Facebook feed and checking for the best spot to set up on the beach more than I'm checking email. This is freaking vacation, and I needed this from the bottom of those rubbed feet to the tip of my soul. I'm tan! Like not tan mom tan, but I've definitely been whiter, so this counts. This is cornier than I get, but the refreshment that this week away is bringing to our family after a month of problem solving and worrying and making excuses and trying and hoping - the kind of stress that exacerbates back pain and turns a typically happy family into a tired and confused family - the relief of this vacation has alleviated all of that. We didn't just pack up that worry and stick it on our doorstep to wait for our return, we let it go. We got our answers before we left and we decided to forget about life for a while. There's still treatments and medicines down here, but there's comfort in knowing that his lungs are ok. He's doing ok and we're doing ok. Actually we are doing freaking awesome. Charleston for the win!
That dropping FEV1 is just a number - as he proclaimed with frustration over the weeks of medications and appointments and attempts to get that number to stop dropping and start improving prior to our departure for this magical vacation - and when we got the results from the bronch and found no bacteria - not even the achromobacter that we've been treating for the past few years - we moved to the other side of worry. As predicted, fungus seems to be the culprit, and an oral anti-fungal medication for the next few months will hopefully help to shift that dial back toward a higher number, but he is well. When we return we will talk to our doctors and make a plan and keep on swimming. For now, I'm putting in a vote for more vacation.
Thursday, July 28, 2016
Your vote counts
This post is an ask for your vote for me, as President of the....wait, wrong topic.
I'm darn proud of the work that I do and I'm even prouder to share that I've been nominated for it as a leader in the Health Activist category by Health 2.0 Conference, the leading showcase of cutting edge innovation that's transforming health and healthcare. I'm listed among many of great ePatient leaders that I'm also proud to call my friends and know that whoever is chosen to represent the collective ePatient voice will do us proud. I'd also feel quite proud if I was chosen as that leader. Voting ends this Sunday, so if you have a moment to spare, your vote for me, Erin Moore, under the Patient Activist category, would be most appreciated.
Vote Here!
I'm darn proud of the work that I do and I'm even prouder to share that I've been nominated for it as a leader in the Health Activist category by Health 2.0 Conference, the leading showcase of cutting edge innovation that's transforming health and healthcare. I'm listed among many of great ePatient leaders that I'm also proud to call my friends and know that whoever is chosen to represent the collective ePatient voice will do us proud. I'd also feel quite proud if I was chosen as that leader. Voting ends this Sunday, so if you have a moment to spare, your vote for me, Erin Moore, under the Patient Activist category, would be most appreciated.
Vote Here!
Wednesday, July 20, 2016
74
I figured out what happened with the Ativan that we were trying to get for Drew's PICC placement last week. His doctor had tried to place the order for it through EPIC for me to pick up at the local pharmacy but because its a controlled substance, you need to physically pick up the prescription from the doctors office and hand the paper to the pharmacist in order to have it filled. Keep in mind that I was getting .25ml, a quarter of a milliliter of Ativan, to help a kid relax. When I had her paged from the pharmacy at the hospital, after searching high and low for the prescription she told me she had called in, to send a new prescription down while she was in the middle of a clinic, she didn't have the option to send, but only to print. Even within the hospital, she couldn't send an order for .25ml of Ativan to the pharmacy for me to pick up to give to him. You may wonder why they didn't just have her order it and have someone from the hospital administer the medication while he was in the OR for the PICC? Well, there isn't a doctor or nurse whose care hes under unless he's admitted to the hospital. So for an outpatient procedure like a PICC placement, the only way we can swing it is for me to get the medicine and take responsibility for him when I give it to him. If only the different parts that make this whole work would talk to one another before making arbitrary rules. This system is so f'd up. I digress.
As I've blogged about before, we've survived a week on IVs. That means dosing at 7am, 8am, 3pm and 11pm - cleaning hands, putting on gloves, cleaning trays, scrubbing the PICC, counting supplies, hooking up the medication, letting it run for an hour, cleaning the PICC again and then tucking it away until the next dose. Add to that mix phone calls from the pharmacy and nurses about levels of medication in his bloodwork, schedules for deliver of new medication and supplies, nurse visits to change the dressing on the PICC and draw labs, and the other interruptions of everyday life. I shouldn't complain about being tired because he sits through all of this and takes it like a champ. There is no swimming, no running around, no sweating. We play games or watch movies, but its a whole lot of inactivity and boredom for a 6yr old.
The hardest part this time around is trying to convince him to take one more medicine, to do one more treatment, interrupting his play to sit through one more dose of IVs when he's feeling absolutely fine. We try to explain that we are doing this to try to get his lungs healthy, to try to get that number back up, and he cries and tells us its not gonna work, mostly because all we've done so far hasn't worked. Maybe he can feel that nothing is changing, or maybe he's just frustrated like us. Either way, its hard to get him to do this all when he doesn't feel like anything is wrong.
What's most disappointing here, and alarming, is that his numbers continue to drop. His normal lung function is in the mid 90's. In the middle of June it was down to 87. Then we tried an oral antibiotic and rechecked and it had gone down to 79. We tried a week on a steroid and it went down to 78. The we went in for the kill with the IV's and after a week, I'm sad to report that he's now down to 74. He's down 20 points in 4 weeks and that's not cool. Just for reference, typically around 30% lung function is when people are discussing the options for transplant.
It's so hard in CF to determine the cause of the problem, like a constant crap shoot. I usually know the symptoms that merit an intervention, whether its a steroid or some IV's, and he hasn't shown signs of needing either of these things this time. We know his lungs are colonized with a drug resistant bacteria called Achromombacter but that doesn't seem to be whats currently causing the problem, otherwise the many different stabs we've taken at this problem would have likely caused the decline to stop, and hopefully turn the other direction. I've had a suspicion from the start that there could be a fungus causing this problem. The last time he had a bronchoscopy, he cultured a lot of fungus in his lungs. People with CF get fungus in their lungs sometimes, and we got it. Was it because he's always on an inhaled antibiotic that he needs to treat symptoms? Did it come from the inhaled steroids he's been on to help him go longer stretches with good health? Is it just something in the environment that he caught because that's how unfortunate having CF can sometimes be? We have no idea. We treated it with 3 months of an anti-fungal medication called fluconazole and it seemed to help his ever so slight increase in cough go away. The thing was that there were no symptoms that alerted us to the fact that he had this problem in his lungs. Last year he wasn't yet doing pulmonary function tests to tell his how his lungs were functioning because he was too young. But could this again be the culprit? Could the fungus we treated have not really actually gone away and now be causing this rapid decline in his lung function? It's our next best guess but there's only one way to find out - time for another bronchscopy.
When Drew learns to cough out the mucus his body produces, we will be able to take a sample of that to the lab to get tested to see specifically what type of bacteria and fungus grows in his airways and more specifically target therapies to help him. Until he is able to do that, he has this procedure done called a bronchoscopy where they put him to sleep, and they squirt saline liquid into his lungs to "wash" them and then suck out the water and test it to see what kind of bacteria or fungus they've found. We can't do this when he's on IV medication or an anti-fungal or the medication will skew the results of the test. So effective today, we stopped all antibiotics and will take him in for a bronchoscopy on Friday afternoon to see if we can figure out what else could be in his lungs that we are missing, and then hopefully figure out how to treat it.
I spent two hours with his doctor yesterday talking through all the options and symptoms and possible outcomes, and I requested that we start him on this anti-fungal drug and think about the bronch when we return from vacation, something we are scheduled to leave for this coming Saturday. She didn't want to start him on something for fear that when we return and do the bronch it wouldn't give us a true picture of what's really going on because of the medication in his system. She also didn't want to wait much longer to try to get to the bottom of this because losing lung function this quickly just isn't good. She also put him back on the steroid with the hope that we can knock out some of the inflammation before the bronch to try to get a really good wash of his lungs, stating that there was little risk [except to his life as me or one of the other kids might strangle the devil child he becomes when he's on a steroid] associated to trying the steroid for another short period of time.
In the meantime, Drew is acting perfectly fine. You would have no idea that anything was going on with him, as he's skipping around here just happy as can be, a little annoyed and sad that he's gotta do so many treatments and take so many pills right now, but otherwise with his normally cheerful and passive attitude about life. I'm hopeful that we will figure this out and be able to regain much of the lost lung function with the right treatment. While we won't have results on Friday since it takes time for a culture to grow, we will have a different treatment option to try and will have answers (hopefully) the following week. Regardless of whether they are good or bad, at least we should have a better idea of what we are dealing with. Thanks for all the thoughts and prayers. While we can't answer everyone individually, know that we appreciate the support and well wishes and will try to keep you posted as we know more!
As I've blogged about before, we've survived a week on IVs. That means dosing at 7am, 8am, 3pm and 11pm - cleaning hands, putting on gloves, cleaning trays, scrubbing the PICC, counting supplies, hooking up the medication, letting it run for an hour, cleaning the PICC again and then tucking it away until the next dose. Add to that mix phone calls from the pharmacy and nurses about levels of medication in his bloodwork, schedules for deliver of new medication and supplies, nurse visits to change the dressing on the PICC and draw labs, and the other interruptions of everyday life. I shouldn't complain about being tired because he sits through all of this and takes it like a champ. There is no swimming, no running around, no sweating. We play games or watch movies, but its a whole lot of inactivity and boredom for a 6yr old.
The hardest part this time around is trying to convince him to take one more medicine, to do one more treatment, interrupting his play to sit through one more dose of IVs when he's feeling absolutely fine. We try to explain that we are doing this to try to get his lungs healthy, to try to get that number back up, and he cries and tells us its not gonna work, mostly because all we've done so far hasn't worked. Maybe he can feel that nothing is changing, or maybe he's just frustrated like us. Either way, its hard to get him to do this all when he doesn't feel like anything is wrong.
What's most disappointing here, and alarming, is that his numbers continue to drop. His normal lung function is in the mid 90's. In the middle of June it was down to 87. Then we tried an oral antibiotic and rechecked and it had gone down to 79. We tried a week on a steroid and it went down to 78. The we went in for the kill with the IV's and after a week, I'm sad to report that he's now down to 74. He's down 20 points in 4 weeks and that's not cool. Just for reference, typically around 30% lung function is when people are discussing the options for transplant.
It's so hard in CF to determine the cause of the problem, like a constant crap shoot. I usually know the symptoms that merit an intervention, whether its a steroid or some IV's, and he hasn't shown signs of needing either of these things this time. We know his lungs are colonized with a drug resistant bacteria called Achromombacter but that doesn't seem to be whats currently causing the problem, otherwise the many different stabs we've taken at this problem would have likely caused the decline to stop, and hopefully turn the other direction. I've had a suspicion from the start that there could be a fungus causing this problem. The last time he had a bronchoscopy, he cultured a lot of fungus in his lungs. People with CF get fungus in their lungs sometimes, and we got it. Was it because he's always on an inhaled antibiotic that he needs to treat symptoms? Did it come from the inhaled steroids he's been on to help him go longer stretches with good health? Is it just something in the environment that he caught because that's how unfortunate having CF can sometimes be? We have no idea. We treated it with 3 months of an anti-fungal medication called fluconazole and it seemed to help his ever so slight increase in cough go away. The thing was that there were no symptoms that alerted us to the fact that he had this problem in his lungs. Last year he wasn't yet doing pulmonary function tests to tell his how his lungs were functioning because he was too young. But could this again be the culprit? Could the fungus we treated have not really actually gone away and now be causing this rapid decline in his lung function? It's our next best guess but there's only one way to find out - time for another bronchscopy.
When Drew learns to cough out the mucus his body produces, we will be able to take a sample of that to the lab to get tested to see specifically what type of bacteria and fungus grows in his airways and more specifically target therapies to help him. Until he is able to do that, he has this procedure done called a bronchoscopy where they put him to sleep, and they squirt saline liquid into his lungs to "wash" them and then suck out the water and test it to see what kind of bacteria or fungus they've found. We can't do this when he's on IV medication or an anti-fungal or the medication will skew the results of the test. So effective today, we stopped all antibiotics and will take him in for a bronchoscopy on Friday afternoon to see if we can figure out what else could be in his lungs that we are missing, and then hopefully figure out how to treat it.
I spent two hours with his doctor yesterday talking through all the options and symptoms and possible outcomes, and I requested that we start him on this anti-fungal drug and think about the bronch when we return from vacation, something we are scheduled to leave for this coming Saturday. She didn't want to start him on something for fear that when we return and do the bronch it wouldn't give us a true picture of what's really going on because of the medication in his system. She also didn't want to wait much longer to try to get to the bottom of this because losing lung function this quickly just isn't good. She also put him back on the steroid with the hope that we can knock out some of the inflammation before the bronch to try to get a really good wash of his lungs, stating that there was little risk [except to his life as me or one of the other kids might strangle the devil child he becomes when he's on a steroid] associated to trying the steroid for another short period of time.
In the meantime, Drew is acting perfectly fine. You would have no idea that anything was going on with him, as he's skipping around here just happy as can be, a little annoyed and sad that he's gotta do so many treatments and take so many pills right now, but otherwise with his normally cheerful and passive attitude about life. I'm hopeful that we will figure this out and be able to regain much of the lost lung function with the right treatment. While we won't have results on Friday since it takes time for a culture to grow, we will have a different treatment option to try and will have answers (hopefully) the following week. Regardless of whether they are good or bad, at least we should have a better idea of what we are dealing with. Thanks for all the thoughts and prayers. While we can't answer everyone individually, know that we appreciate the support and well wishes and will try to keep you posted as we know more!
This video was taken 15min before I wrote this post - as you can see he seems to be feeling just fine!
Tuesday, July 12, 2016
Crazytown
I'm hoping that this brain dump will alleviate my headache. God its been a long couple of days. We went back to Children's yesterday for a PFT to check Drew's lung function post-steroid and to determine if he would need IV antibiotics. I knew that the steroids weren't working, but held out hope that we wouldn't need IV's. He blew a 77 this time, down again. We went from 92 in March, to 85 in early June, to 79 two weeks ago and we're now down to 77. The mystery of it all is that he remains symptom-less. I've been wracking my brain trying to figure out what could possibly be wrong since this is completely uncharacteristic of an "exacerbation" for Drew. I have an exacerbation score sheet for godsake and it's telling me that he is not having an exacerbation, despite lung function that continues to drop lower and lower. All of this thought and wonder and worry culminated in the parking lot of Home Depot on Sunday where I sat crying because I couldn't find a paint color for my living room. My cure for grief is action, and so despite being mentally and physically exhausted, I decided that we needed to paint the house. So we did. (I finally found the right paint color and we got that all taken care of on Sunday, in case you were wondering).
We had talked to Drew's doctor over the weekend about our plan for if his numbers were still low, and had scheduled an appointment to have a PICC placed at 10am on Monday, something that we could easily cancel if his numbers were miraculously up. They weren't, and so at 7:45 on Monday morning we knew our plan. We had discussed what medications we would use, the dosing schedule, the plan for the PICC placement - no sedation, just a small dose of Ativan to keep him calm (next time i'm asking for a dose for me too) - and we were set. A wonderful friend who is going to make a wonderful doctor someday soon met us at the hospital to keep us company and better understand the patient and family experience of care through this process. I was so grateful to have her with us when the first hiccup of the day happened.
Drew was scheduled for his PICC at 10am, and I was to pick up his dose of Ativan at the hospital pharmacy that morning. When we arrived at 7:30, I realized that that pharmacy didn't open until 9am, no problem. After we got the results of the PFT and knew that the PICC was a go, we went down to radiology to register for the PICC procedure and were quickly ushered back to an isolation waiting room, something I request the moment we step foot into the hospital. For me, there is always a fear of a[nother] hospital acquired drug resistant infection, so I take extra steps to ensure his safety and my comfort with it. The issue I have with these so-called "isolation rooms" is that there is no indication of when it's been cleaned. I don't know who was in it before me, whether it's been cleaned, if it will be cleaned when I leave it, or anything at all about its cleanliness. I do not trust blindly, especially when it comes to Drew and germs. Can't we put a sign on the door to indicate that the room is clean? Anyway, we got called right up to interventional radiology so they could use an ultrasound machine to identify a good place in his arm to put the PICC and then mark it and add numbing cream. The nurse then took us back to the isolation room - the one we had been in, the one that I had closed the door to before we went upstairs for a moment but when we returned the door had been opened, the one I had no indication of having remained ours and no one elses while we were gone for 20 minutes - to wait for the pharmacy to open so we could get his dose of Ativan before starting the procedure. She told me to have the receptionist page her when we got the medication and were ready, as it looked likely that they could take us early.
So at 9am, I left my friend with Drew in the isolation room to run over to the pharmacy to pick up the medication, only they didn't have it. Did I screw up? Was I supposed to have gotten it from CVS on my way in? I had her call CVS to see if they had it and could transfer the prescription, but they didn't have it either. His doctor had emailed me yesterday to say she had called it in, and I was able to pick of the other anti-nausea medicine, but the Ativan was nowhere to be found. I called up to clinic and had the receptionist page the nurse who was covering for our nurse who is on vacation. She told me she would page Drew's doctor, who is in clinic seeing patients, to have her call down a new prescription as soon as possible. At 9:40, forty minutes after having arrived in the pharmacy to pick up this order and delaying the process of getting a PICC, something that was suggested by my husband that perhaps I try without the Ativan so as to not delay the placement of the PICC any longer, the pharmacy got the order and gave me the med. I was livid. I was livid not because of the mix up, though I don't know what happened to the first order, but because I was already exhausted - mentally and emotionally, trying to prepare myself and Drew and our family for what life will be like for the next two weeks with running IVs from home, with no swimming, with no sweating, with lots of interruptions from pharmacies and home care nurses and extra appointments and a rigid schedule of medication infusions - and now I had to become the detective and problem solver of a problem that I had no part in creating. Sure, I could have walked away and we could have done the PICC without the Ativan, but to help him, if even just a little, relax and feel a tiny bit more at ease about the whole process was worth the work. The longer it took to get the medicine, the more my stress levels rose. He was waiting, nervously, without me in a room with a friend of mine he only kind of knows while I asked and waited and tried to decide which direction to go. Thankfully I stayed and got the medicine, because the PICC placement didn't go as planned - 6 sticks, two blown PICCs and finally a successful placement later and we were all set. Without the Ativan, this would have been suffering. Avoidable, minimizable suffering that has a lasting impact on a kid who already has more to deal with than most adults will in their lifetime. I will always request Ativan, not because he needs it, but because he deserves it.
Following the PICC placement procedure, we went back up to clinic to meet with the homecare nurse for the first doses of the medication. We always do this at the hospital in case there is a reaction. IV's are no joke, and its better to be safe than sorry. Our nurse was lovely and we chatted while I answered a flurry of text messages from concerned friends and family members. Drew happily colored and played on his iPod until the first two infusions were done, and we were on our way home by 3pm. To think of this as a short day was a bit ironic given that we had arrived at 7:30am, but sometimes these days can last for 12 or 15 hours, so this felt short. It felt short anyway until we got home. Then it hit me like a brick wall. We had made it, I could exhale, and the stress of the unknown from the past several weeks started to show up in my horrible back pain, throbbing headache, and exhausted mind. I laid on the couch for the next many hours, my husband putting the kids to bed, and then finally went to bed myself after hooking him up to his nighttime dose of Meropenum. I woke up today feeling awful. My head hurts. My everything hurts. I don't know if its harder this time because he's more aware of what's happening and in addition to managing my own stress and anxiety about everything I'm also trying to minimize his? Is it because the rest of the family sees this as unfair and I feel responsibility to help manage expectation and disappointments and frustrations? I don't know. I do know that in a day or two we will find our groove, everyone will have accepted our temporary routine. Forgive our messy house and scattered minds and shitty attitudes for the next two weeks. It's sort of like survival mode over here, for all of us. We so greatly appreciate all of the thoughts and prayers, and will keep you updated on all things happening here in crazytown.
We had talked to Drew's doctor over the weekend about our plan for if his numbers were still low, and had scheduled an appointment to have a PICC placed at 10am on Monday, something that we could easily cancel if his numbers were miraculously up. They weren't, and so at 7:45 on Monday morning we knew our plan. We had discussed what medications we would use, the dosing schedule, the plan for the PICC placement - no sedation, just a small dose of Ativan to keep him calm (next time i'm asking for a dose for me too) - and we were set. A wonderful friend who is going to make a wonderful doctor someday soon met us at the hospital to keep us company and better understand the patient and family experience of care through this process. I was so grateful to have her with us when the first hiccup of the day happened.
Drew was scheduled for his PICC at 10am, and I was to pick up his dose of Ativan at the hospital pharmacy that morning. When we arrived at 7:30, I realized that that pharmacy didn't open until 9am, no problem. After we got the results of the PFT and knew that the PICC was a go, we went down to radiology to register for the PICC procedure and were quickly ushered back to an isolation waiting room, something I request the moment we step foot into the hospital. For me, there is always a fear of a[nother] hospital acquired drug resistant infection, so I take extra steps to ensure his safety and my comfort with it. The issue I have with these so-called "isolation rooms" is that there is no indication of when it's been cleaned. I don't know who was in it before me, whether it's been cleaned, if it will be cleaned when I leave it, or anything at all about its cleanliness. I do not trust blindly, especially when it comes to Drew and germs. Can't we put a sign on the door to indicate that the room is clean? Anyway, we got called right up to interventional radiology so they could use an ultrasound machine to identify a good place in his arm to put the PICC and then mark it and add numbing cream. The nurse then took us back to the isolation room - the one we had been in, the one that I had closed the door to before we went upstairs for a moment but when we returned the door had been opened, the one I had no indication of having remained ours and no one elses while we were gone for 20 minutes - to wait for the pharmacy to open so we could get his dose of Ativan before starting the procedure. She told me to have the receptionist page her when we got the medication and were ready, as it looked likely that they could take us early.
So at 9am, I left my friend with Drew in the isolation room to run over to the pharmacy to pick up the medication, only they didn't have it. Did I screw up? Was I supposed to have gotten it from CVS on my way in? I had her call CVS to see if they had it and could transfer the prescription, but they didn't have it either. His doctor had emailed me yesterday to say she had called it in, and I was able to pick of the other anti-nausea medicine, but the Ativan was nowhere to be found. I called up to clinic and had the receptionist page the nurse who was covering for our nurse who is on vacation. She told me she would page Drew's doctor, who is in clinic seeing patients, to have her call down a new prescription as soon as possible. At 9:40, forty minutes after having arrived in the pharmacy to pick up this order and delaying the process of getting a PICC, something that was suggested by my husband that perhaps I try without the Ativan so as to not delay the placement of the PICC any longer, the pharmacy got the order and gave me the med. I was livid. I was livid not because of the mix up, though I don't know what happened to the first order, but because I was already exhausted - mentally and emotionally, trying to prepare myself and Drew and our family for what life will be like for the next two weeks with running IVs from home, with no swimming, with no sweating, with lots of interruptions from pharmacies and home care nurses and extra appointments and a rigid schedule of medication infusions - and now I had to become the detective and problem solver of a problem that I had no part in creating. Sure, I could have walked away and we could have done the PICC without the Ativan, but to help him, if even just a little, relax and feel a tiny bit more at ease about the whole process was worth the work. The longer it took to get the medicine, the more my stress levels rose. He was waiting, nervously, without me in a room with a friend of mine he only kind of knows while I asked and waited and tried to decide which direction to go. Thankfully I stayed and got the medicine, because the PICC placement didn't go as planned - 6 sticks, two blown PICCs and finally a successful placement later and we were all set. Without the Ativan, this would have been suffering. Avoidable, minimizable suffering that has a lasting impact on a kid who already has more to deal with than most adults will in their lifetime. I will always request Ativan, not because he needs it, but because he deserves it.
Following the PICC placement procedure, we went back up to clinic to meet with the homecare nurse for the first doses of the medication. We always do this at the hospital in case there is a reaction. IV's are no joke, and its better to be safe than sorry. Our nurse was lovely and we chatted while I answered a flurry of text messages from concerned friends and family members. Drew happily colored and played on his iPod until the first two infusions were done, and we were on our way home by 3pm. To think of this as a short day was a bit ironic given that we had arrived at 7:30am, but sometimes these days can last for 12 or 15 hours, so this felt short. It felt short anyway until we got home. Then it hit me like a brick wall. We had made it, I could exhale, and the stress of the unknown from the past several weeks started to show up in my horrible back pain, throbbing headache, and exhausted mind. I laid on the couch for the next many hours, my husband putting the kids to bed, and then finally went to bed myself after hooking him up to his nighttime dose of Meropenum. I woke up today feeling awful. My head hurts. My everything hurts. I don't know if its harder this time because he's more aware of what's happening and in addition to managing my own stress and anxiety about everything I'm also trying to minimize his? Is it because the rest of the family sees this as unfair and I feel responsibility to help manage expectation and disappointments and frustrations? I don't know. I do know that in a day or two we will find our groove, everyone will have accepted our temporary routine. Forgive our messy house and scattered minds and shitty attitudes for the next two weeks. It's sort of like survival mode over here, for all of us. We so greatly appreciate all of the thoughts and prayers, and will keep you updated on all things happening here in crazytown.
Friday, July 8, 2016
I'm a maker. We're all makers.
A few weeks ago, I threw a tweet out into the universe looking for good ideas on how to create a hands-free nebulizer for Drew. He gets to play on his iPod during treatments, and with having to hold the nebulizer, he's only got one hand free to play games that mostly require two hands. He does this thing with his arm where he uses it as a ledge to balance the neb, but it usually falls or spills leaving both of us feeling frustrated. A mask would be a simple solution, but we'd graduated from a mask to a mouthpiece for deep breaths and deeper medication penetration into his lungs, and also for the opportunity to utilize the Aerobika for additional positive expiratory pressure, something that helps to open his floppy airways and allow him to cough out the junk that makes him sick. Anyway, you can't use a mask with the Aerobika, so we are left trying to find ways to allow him the simple pleasure of playing on his iPod during treatments while still receiving the full benefit of the treatment.
So a tweet went out, and what transpired was nothing short of magical. People from around the globe and in a variety of industries and roles shared their ideas and feedback on what we could do to solve this problem. I love it when the network uses its powers for good. Read what Susanna Fox captured in this Storify of the weeks we spent online prototyping options and finally reaching a reasonable solution. A solution, I should add, that now lives on the Maker Health website (or will as soon as I hit "publish"). This is a place where anyone with a good idea can share their idea to help others learn. Check it out.
So a tweet went out, and what transpired was nothing short of magical. People from around the globe and in a variety of industries and roles shared their ideas and feedback on what we could do to solve this problem. I love it when the network uses its powers for good. Read what Susanna Fox captured in this Storify of the weeks we spent online prototyping options and finally reaching a reasonable solution. A solution, I should add, that now lives on the Maker Health website (or will as soon as I hit "publish"). This is a place where anyone with a good idea can share their idea to help others learn. Check it out.
Here's the deal
In the middle of June, I wrote a post about Drew's clinic visit and declining lung function. His normal range is mid 90's. At our quarterly check up, his number was down to 85. Before we left for Philadelphia he had dropped down to 79. We decided to treat him with 2 weeks of an oral antibiotic to see if that would help him, thinking that there is probably an infection in his lungs (there's always an infection in his lungs, like literally, but its not always causing a problem), and planned to retest him upon our return. Well, we returned and his lung function is still at 79.
So the big question is what to do. Normally, I would be on board for treatment. But normally he would be "sick" in the more traditional sense - increased cough, decreased appetite and energy level. And none of those things are there. I've used my Orchestra data to tell the story of his health time and time again, and i'm coming up short this time. There is no cough, and there hasn't been for months. His weight is better than its ever been, and his appetite remains unchanged. He is sleeping well and generally happy. Yet his lung function is going down. His doctor suggested that sometimes kids this age aren't able to articulate when they can't quite take as deep a breath, or when they're struggling to clear secretions when they have a more subtle infection going on, stuff that may be less obvious to my naked ear. But I feel like he would have something going on that I would notice, anything, and I don't. Sometimes people with CF just need a tune-up, and I hate prolonging the inevitable if that's what needs to happen. The thing is, I'm not convinced that's what needs to happen. I don't know what the problem is - an infection? increased inflammation? allergies? reflux? I don't know, and the only way that it would seem that we can figure that out is to try different treatment options to see how he responds to them and what makes him better.
The current plan is a steroid burst to see if there is inflammation that we can get under control, and retesting his lung function on Monday morning. We also have an appointment to have a PICC placed on Monday morning following the PFT to start two weeks on IVs if his numbers aren't up. Hopefully one of these things work. Normally I'm annoyed when people try to give me suggestions for how to treat him because I normally feel like I have a pretty good handle on him as an individual, but this time I am at a loss. I don't know whats going on. I don't have data to support any theory of illness or allergy or other inflammation otherwise. I'm open to ideas, thoughts and suggestions so please do send them my way if you have them. Stay tuned!
So the big question is what to do. Normally, I would be on board for treatment. But normally he would be "sick" in the more traditional sense - increased cough, decreased appetite and energy level. And none of those things are there. I've used my Orchestra data to tell the story of his health time and time again, and i'm coming up short this time. There is no cough, and there hasn't been for months. His weight is better than its ever been, and his appetite remains unchanged. He is sleeping well and generally happy. Yet his lung function is going down. His doctor suggested that sometimes kids this age aren't able to articulate when they can't quite take as deep a breath, or when they're struggling to clear secretions when they have a more subtle infection going on, stuff that may be less obvious to my naked ear. But I feel like he would have something going on that I would notice, anything, and I don't. Sometimes people with CF just need a tune-up, and I hate prolonging the inevitable if that's what needs to happen. The thing is, I'm not convinced that's what needs to happen. I don't know what the problem is - an infection? increased inflammation? allergies? reflux? I don't know, and the only way that it would seem that we can figure that out is to try different treatment options to see how he responds to them and what makes him better.
The current plan is a steroid burst to see if there is inflammation that we can get under control, and retesting his lung function on Monday morning. We also have an appointment to have a PICC placed on Monday morning following the PFT to start two weeks on IVs if his numbers aren't up. Hopefully one of these things work. Normally I'm annoyed when people try to give me suggestions for how to treat him because I normally feel like I have a pretty good handle on him as an individual, but this time I am at a loss. I don't know whats going on. I don't have data to support any theory of illness or allergy or other inflammation otherwise. I'm open to ideas, thoughts and suggestions so please do send them my way if you have them. Stay tuned!
Sunday, June 19, 2016
My ideal
We had an appointment this morning and it went great! We woke up early and did all of our breathing treatments, and right before they ended, we signed onto our web portal so that our respiratory therapist could watch how we do them and review settings on the vest. We both took some notes. We discussed using a new device called an Aerobika, something that he can breath into that will give positive pressure and vibration so loosen secretions which he can then expel. She shares a link for us to check out another kid using it on YouTube and tells us she will send one out with home care later this afternoon.
Between the RT and the doctor, our nurse gets online to review our current meds with us. She's sent me a message through our shared portal last week and asked me to review, marking the medications that we are or are not taking, and I'm able to do it one evening after I get the kids to bed. She simply confirms that nothing has changed before we move on. She asks what we need from them - refills, doctors notes, referrals - and agrees to email us the forms I had sent for school next year, and then steps away to grab the doctor.
The doctor pops on to review labs that we had done at the outpatient clinic one evening last week and is pleased that everything looks great. We've been practicing our PFTs with our home spirometer and, while our number is down slightly, we agree that since everything else is going so well that we should just stop by the clinic sometime this coming week to repeat it in the PFT lab to make sure there isn't something going on that needs treating. His weight looks great, something she's been following through our shared tracking portal, and neither of us feels the need to meet with the dietician this visit. We had discussed this prior to our visit in our pre-visit plan, but she confirmed that he was in good standing all around and agreed it wasn't necessary to spend time meeting with anyone else. As she is talking, we both have the opportunity to create a shared note - her turning my narrative into data and me reacting her thoughts and turning her suggestions into action items in my own words. She notices that my interpretation of what she had said earlier wasn't what she had meant, and we quickly discuss before we both feel confident in our next step. She asks about our summer plans and what refills we might need, and then puts us on a brief hold while transferring us to the Infectious Disease doctor whose following us because of Drew's achromobacter.
After just a few minutes on hold, the ID doc gets on the line with his nurse and we talk about next steps for treating his achromobacter and candida, a fungus that grew on his last culture. We have culture swabs at home that we use every few months and mail them into the lab so that we have results to discuss during our visit. This is so much better than the old way when there would be an anxiety filled week waiting for a lab result to pop up in MyChart, not knowing what it would say or how it would or wouldn't change our life. We know what he's got going on down there, and talk about plans for treatment. He mentions a study currently underway for CF kids looking at the variety of bacteria families found within one persons airway to determine if folks are acquiring one strain of a bacteria or multiple, and has found that in the 80ish folks they've tested, not only do they only have one strain, but they're all unique, suggesting that the infection control protocols they've put in place have all but eliminated the passing of bacteria from person to person in clinic. This is good news for a germophobe to hear! He offers to take a look at the specific strains of achromobacter that Drew has to determine how they act and react to different medications, and naturally I take him up on the offer. The notes I'm taking that he can see are reminders for myself to discuss with my husband when we he gets home this evening.
Before we get off the call, the nurse who had joined the ID doc offers to help us arrange our next appointment, suggesting that it may be difficult to find a time that works with everyone schedules. She shares her screen while I look through my calendar and we are able to find something that works.
Before we hang up, we are scheduled for our next follow up, this one will be in person as we alternate between e-visits and visits to the hospital to minimize the interruption that CF has in our lives and also the risk to catching something while we are there. We can both download a copy of note we have co-created. The appointment is over within 45 minutes, taking approximately 2-3 hours off the time of a normal visit. Drew is excited to have seen the faces of the folks who normally take care of them, as over video conference they don't need to gown, glove and mask. Its funny how a little face time, even virtually, can create that kind of connection.
None of this really happened. But what if? What if I didn't have to find a babysitter for the other kids during Drew's appointments, paying them for 4 hours while I sit in clinic with Drew who would rather be at home. What if I didn't have to bribe him with treats for not touching the elevator buttons in the hospital. What if I could get labs done in the evening rather than between 9-4, and what if I could talk with my doctor about the result the same day that the results come in, eliminating much of the worry and fear that comes simply with waiting. What if I had the chance to modify his med list, telling them what we take, and ensuring its correctness in his medical record, in real time. What if I could really create a note with his doctor, google docs style - me typing in blue and her in red, the respiratory therapist in orange and the dietician in green and the infectious disease doc in purple, true and total transparency - and what if that enhanced understanding between us, me more clearly understanding her recommendations, and her having a glimpse into my thoughts and feelings, practical and emotional, eliminating errors and misunderstandings, creating an action plan that we both feel confident that we can follow. What if I could look at a calendar online at a time that's convenient for me, selecting who I want to see and when, simultaneously checking my calendar to find a time that works for us and never having to wait on hold while a scheduler tries to solve this for me between the hours of 9-4pm.
What really happened during our appointment last week was captured in the previous post, but if I had it my way, this would be my ideal.
Between the RT and the doctor, our nurse gets online to review our current meds with us. She's sent me a message through our shared portal last week and asked me to review, marking the medications that we are or are not taking, and I'm able to do it one evening after I get the kids to bed. She simply confirms that nothing has changed before we move on. She asks what we need from them - refills, doctors notes, referrals - and agrees to email us the forms I had sent for school next year, and then steps away to grab the doctor.
The doctor pops on to review labs that we had done at the outpatient clinic one evening last week and is pleased that everything looks great. We've been practicing our PFTs with our home spirometer and, while our number is down slightly, we agree that since everything else is going so well that we should just stop by the clinic sometime this coming week to repeat it in the PFT lab to make sure there isn't something going on that needs treating. His weight looks great, something she's been following through our shared tracking portal, and neither of us feels the need to meet with the dietician this visit. We had discussed this prior to our visit in our pre-visit plan, but she confirmed that he was in good standing all around and agreed it wasn't necessary to spend time meeting with anyone else. As she is talking, we both have the opportunity to create a shared note - her turning my narrative into data and me reacting her thoughts and turning her suggestions into action items in my own words. She notices that my interpretation of what she had said earlier wasn't what she had meant, and we quickly discuss before we both feel confident in our next step. She asks about our summer plans and what refills we might need, and then puts us on a brief hold while transferring us to the Infectious Disease doctor whose following us because of Drew's achromobacter.
After just a few minutes on hold, the ID doc gets on the line with his nurse and we talk about next steps for treating his achromobacter and candida, a fungus that grew on his last culture. We have culture swabs at home that we use every few months and mail them into the lab so that we have results to discuss during our visit. This is so much better than the old way when there would be an anxiety filled week waiting for a lab result to pop up in MyChart, not knowing what it would say or how it would or wouldn't change our life. We know what he's got going on down there, and talk about plans for treatment. He mentions a study currently underway for CF kids looking at the variety of bacteria families found within one persons airway to determine if folks are acquiring one strain of a bacteria or multiple, and has found that in the 80ish folks they've tested, not only do they only have one strain, but they're all unique, suggesting that the infection control protocols they've put in place have all but eliminated the passing of bacteria from person to person in clinic. This is good news for a germophobe to hear! He offers to take a look at the specific strains of achromobacter that Drew has to determine how they act and react to different medications, and naturally I take him up on the offer. The notes I'm taking that he can see are reminders for myself to discuss with my husband when we he gets home this evening.
Before we get off the call, the nurse who had joined the ID doc offers to help us arrange our next appointment, suggesting that it may be difficult to find a time that works with everyone schedules. She shares her screen while I look through my calendar and we are able to find something that works.
Before we hang up, we are scheduled for our next follow up, this one will be in person as we alternate between e-visits and visits to the hospital to minimize the interruption that CF has in our lives and also the risk to catching something while we are there. We can both download a copy of note we have co-created. The appointment is over within 45 minutes, taking approximately 2-3 hours off the time of a normal visit. Drew is excited to have seen the faces of the folks who normally take care of them, as over video conference they don't need to gown, glove and mask. Its funny how a little face time, even virtually, can create that kind of connection.
None of this really happened. But what if? What if I didn't have to find a babysitter for the other kids during Drew's appointments, paying them for 4 hours while I sit in clinic with Drew who would rather be at home. What if I didn't have to bribe him with treats for not touching the elevator buttons in the hospital. What if I could get labs done in the evening rather than between 9-4, and what if I could talk with my doctor about the result the same day that the results come in, eliminating much of the worry and fear that comes simply with waiting. What if I had the chance to modify his med list, telling them what we take, and ensuring its correctness in his medical record, in real time. What if I could really create a note with his doctor, google docs style - me typing in blue and her in red, the respiratory therapist in orange and the dietician in green and the infectious disease doc in purple, true and total transparency - and what if that enhanced understanding between us, me more clearly understanding her recommendations, and her having a glimpse into my thoughts and feelings, practical and emotional, eliminating errors and misunderstandings, creating an action plan that we both feel confident that we can follow. What if I could look at a calendar online at a time that's convenient for me, selecting who I want to see and when, simultaneously checking my calendar to find a time that works for us and never having to wait on hold while a scheduler tries to solve this for me between the hours of 9-4pm.
What really happened during our appointment last week was captured in the previous post, but if I had it my way, this would be my ideal.
Tuesday, June 14, 2016
Yesterdays appointment, and problems with the system
Drew had a clinic visit yesterday and it went pretty well! We haven't been to clinic for about 4 months because I didn't want to pull him out of school for an appointment, so with good health, we pushed it out an extra month and went just yesterday. He's been incredibly healthy for the past 18 months, a longer stretch of time without any oral or IV medications than he's ever had which is amazing. His PFTs were low yesterday - not so low that any action needed to be taken but low enough to cause some concern from his doc. But here's the thing - I've seen him do his PFTs before, and while he's still relatively new to the process, he wasn't doing them quite right. I can't put my finger on exactly how it was different, but he wasn't blasting all his breath as hard as he could right off the bat, and I don't think its because he couldn't due to an illness. When he does his breathing treatments at home, he uses a device called an Aerobika that he blows into with long, hard blows that cause a positive pressure in his lungs and opens them up (hes got malacia that makes them extra floppy) and allows him to move mucus. I think he's got the Aerobika technique mixed up with the PFT technique and I'm not sure how to fix it. We are going to come back in two weeks to try again.
Otherwise, the appointment was pretty unremarkable. He's gaining weight like a boss and is happy and healthy and so are we. I'll do a culture this weekend when he's been off of one of his treatments for a few days so we should know more about any new bugs in another week. Fingers crossed we are still just dealing with the beast that is achromobacter. We will also repeat his PFT before we head back to Philly to see if we can get his number back up, and if its still low will have to discuss options to treat or try to figure out what's causing the low number.


Another flaw of the system is appointment scheduling. I need to take Drew back for another appointment in 3 month, and then in 3 months again. I have a preference for the first appointment on a Monday morning, and I also have a preference that we do these appointments at a time that is least disruptive to his life, specifically days off of school. It doesn't matter what anyone else thinks I should do or not do, should deal with or not deal with. This is our life and our preference and we should be allowed to live it according to our own priorities. I digress.
So I called to schedule an appointment for September. In my mind, this should be early enough to schedule an appointment for September 12, a day that he will be off of school. Well there are no appointments available on September 12, only the 19th, and not until later in the morning. So I ask about October, willing to push to the next day off of school so that he's allowed to keep doing what he wants, which is being at school with his buddies and not missing out. Well the schedule for October isn't available yet so I can't schedule for October. I go back to the 19th that they had proposed, however the infectious disease doc that we also see during our appointments isn't available on the 19th so we would have to make a separate appointment to see him. Listen, I don't like to come into a hospital with my kid who is susceptible to dangerous infections in the first place. Now you want me to pull him out of school AND bring him in twice? I'll figure out another solution.
After 12 minutes on the phone I hung up with no appointments and no plan. I can schedule a haircut for my kids from my phone - why can't I log into MyChart and browse through appointment options that work for me? Why does a system that weighs so heavily on patients and families make it so hard to do such simple tasks? What can we do to change this?! And for the record, I don't think these are unreasonable requests. If a motivated, engaged, health-literate adult has this much trouble navigating the system, are we actually maybe causing harm by not addressing these seemingly soft problems?
Otherwise, the appointment was pretty unremarkable. He's gaining weight like a boss and is happy and healthy and so are we. I'll do a culture this weekend when he's been off of one of his treatments for a few days so we should know more about any new bugs in another week. Fingers crossed we are still just dealing with the beast that is achromobacter. We will also repeat his PFT before we head back to Philly to see if we can get his number back up, and if its still low will have to discuss options to treat or try to figure out what's causing the low number.
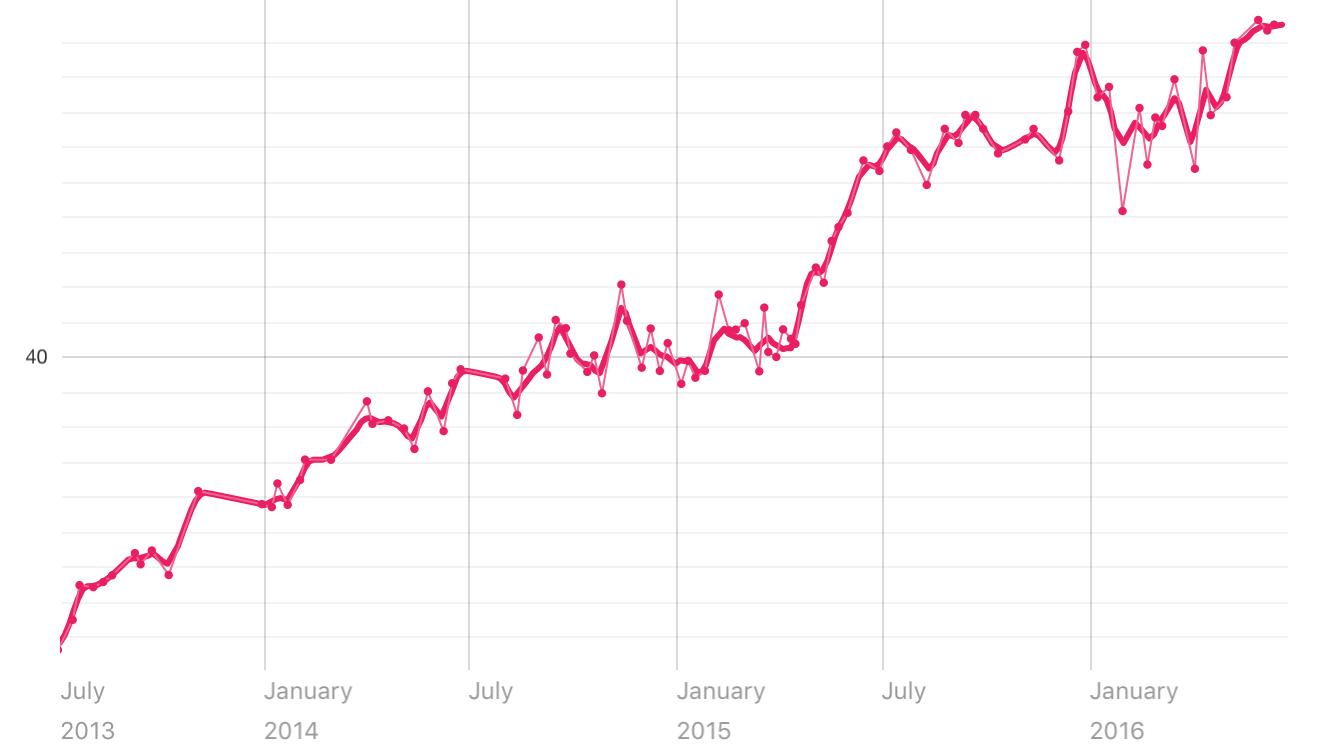
Weight chart from July 2013 to present! BOOM!
The next part of this post is in no way a dig at our hospital or our care team, but rather a general annoyance with the system that I experienced and I've heard many of my peers experience. These are my feelings and opinions and don't reflect that of anyone by myself. And i'm so annoyed that I even stated that.
Per the usual, upon arrival at clinic a nurse or another assistant will come in to take Drew's vitals and then review our med list. And every time, I ask why we are doing it with the response being, "We just want to make sure everything is up to date", though I've yet to see anything change. So we went through the list:
Her: "When was the last time he took Albuterol?"
Me: "4 years ago"
Her: "Atrovent"
Me: "2 years ago"
Her: "Pulmicort"
Me: "6mo ago"
Her: "Azithromycin"
Me: "The liquid or the pill?"
Her: "The liquid"
Me: "3mo"
Her: "The pill?"
Me: "This morning."
Her: "Fluconazole"
Me: "That was just a 3mo treatment"
Her: "So he's off it?"
Me: "Yes"
And on and on and on. We got all the meds hes taking, and "got rid of" the meds he isn't, and we went on with our appointment.
Then before I left, I got my After Visit Summary (AVS), a nice little report of what we discussed during the visit, recommended action steps (make your next appointment, for example), and an updated medication list. Only it's not. Now I don't really care too much whether the med list on my AVS is accurate because I don't use the AVS for much, just a reference or reminder, or to tell my husband what we talked about in clinic. But if it's wrong on my printout, its wrong in my EMR, and the next time I'm asked what med's we are on, we will waste everyone's time by going through this whole process over again. And nothing changes. I've experienced this countless times with homecare nursing, sometimes coming twice a day and having to go through this process, and the list has never, even been right. Before he has gone in for procedures I will review it with someone on the phone the night before, then a nurse in the OR that morning, then again with anesthesia before they take him back and every single time we make the exact same corrections. I think the reason it doesn't change is because only the prescribing physician, the one who put it into the EMR, can take it out, so when you think that the nurse is making the changes they're really just making a note of the changes, flagging them as needing changed, and expecting that the doctor will at some point go in and make the changes. But that doesn't happen, and at no fault of the doc or the nurse or anyone else specifically, except a faulty system. What if something happened to Drew and I wasn't there to tell them what medications he's taking and with what frequency? What if someone less empowered than I used that AVS as a guide for taking their medications? What if there were harmful drug interactions in that list - something new added when the old stuff is never taken away? How might we fix this? The kicker of this image is that is states very clearly that "this list is accurate as of 6/13/16 at 11:59pm". Only it's not.

So I called to schedule an appointment for September. In my mind, this should be early enough to schedule an appointment for September 12, a day that he will be off of school. Well there are no appointments available on September 12, only the 19th, and not until later in the morning. So I ask about October, willing to push to the next day off of school so that he's allowed to keep doing what he wants, which is being at school with his buddies and not missing out. Well the schedule for October isn't available yet so I can't schedule for October. I go back to the 19th that they had proposed, however the infectious disease doc that we also see during our appointments isn't available on the 19th so we would have to make a separate appointment to see him. Listen, I don't like to come into a hospital with my kid who is susceptible to dangerous infections in the first place. Now you want me to pull him out of school AND bring him in twice? I'll figure out another solution.
After 12 minutes on the phone I hung up with no appointments and no plan. I can schedule a haircut for my kids from my phone - why can't I log into MyChart and browse through appointment options that work for me? Why does a system that weighs so heavily on patients and families make it so hard to do such simple tasks? What can we do to change this?! And for the record, I don't think these are unreasonable requests. If a motivated, engaged, health-literate adult has this much trouble navigating the system, are we actually maybe causing harm by not addressing these seemingly soft problems?