We had an appointment this morning and it went great! We woke up early and did all of our breathing treatments, and right before they ended, we signed onto our web portal so that our respiratory therapist could watch how we do them and review settings on the vest. We both took some notes. We discussed using a new device called an Aerobika, something that he can breath into that will give positive pressure and vibration so loosen secretions which he can then expel. She shares a link for us to check out another kid using it on YouTube and tells us she will send one out with home care later this afternoon.
Between the RT and the doctor, our nurse gets online to review our current meds with us. She's sent me a message through our shared portal last week and asked me to review, marking the medications that we are or are not taking, and I'm able to do it one evening after I get the kids to bed. She simply confirms that nothing has changed before we move on. She asks what we need from them - refills, doctors notes, referrals - and agrees to email us the forms I had sent for school next year, and then steps away to grab the doctor.
The doctor pops on to review labs that we had done at the outpatient clinic one evening last week and is pleased that everything looks great. We've been practicing our PFTs with our home spirometer and, while our number is down slightly, we agree that since everything else is going so well that we should just stop by the clinic sometime this coming week to repeat it in the PFT lab to make sure there isn't something going on that needs treating. His weight looks great, something she's been following through our shared tracking portal, and neither of us feels the need to meet with the dietician this visit. We had discussed this prior to our visit in our pre-visit plan, but she confirmed that he was in good standing all around and agreed it wasn't necessary to spend time meeting with anyone else. As she is talking, we both have the opportunity to create a shared note - her turning my narrative into data and me reacting her thoughts and turning her suggestions into action items in my own words. She notices that my interpretation of what she had said earlier wasn't what she had meant, and we quickly discuss before we both feel confident in our next step. She asks about our summer plans and what refills we might need, and then puts us on a brief hold while transferring us to the Infectious Disease doctor whose following us because of Drew's achromobacter.
After just a few minutes on hold, the ID doc gets on the line with his nurse and we talk about next steps for treating his achromobacter and candida, a fungus that grew on his last culture. We have culture swabs at home that we use every few months and mail them into the lab so that we have results to discuss during our visit. This is so much better than the old way when there would be an anxiety filled week waiting for a lab result to pop up in MyChart, not knowing what it would say or how it would or wouldn't change our life. We know what he's got going on down there, and talk about plans for treatment. He mentions a study currently underway for CF kids looking at the variety of bacteria families found within one persons airway to determine if folks are acquiring one strain of a bacteria or multiple, and has found that in the 80ish folks they've tested, not only do they only have one strain, but they're all unique, suggesting that the infection control protocols they've put in place have all but eliminated the passing of bacteria from person to person in clinic. This is good news for a germophobe to hear! He offers to take a look at the specific strains of achromobacter that Drew has to determine how they act and react to different medications, and naturally I take him up on the offer. The notes I'm taking that he can see are reminders for myself to discuss with my husband when we he gets home this evening.
Before we get off the call, the nurse who had joined the ID doc offers to help us arrange our next appointment, suggesting that it may be difficult to find a time that works with everyone schedules. She shares her screen while I look through my calendar and we are able to find something that works.
Before we hang up, we are scheduled for our next follow up, this one will be in person as we alternate between e-visits and visits to the hospital to minimize the interruption that CF has in our lives and also the risk to catching something while we are there. We can both download a copy of note we have co-created. The appointment is over within 45 minutes, taking approximately 2-3 hours off the time of a normal visit. Drew is excited to have seen the faces of the folks who normally take care of them, as over video conference they don't need to gown, glove and mask. Its funny how a little face time, even virtually, can create that kind of connection.
None of this really happened. But what if? What if I didn't have to find a babysitter for the other kids during Drew's appointments, paying them for 4 hours while I sit in clinic with Drew who would rather be at home. What if I didn't have to bribe him with treats for not touching the elevator buttons in the hospital. What if I could get labs done in the evening rather than between 9-4, and what if I could talk with my doctor about the result the same day that the results come in, eliminating much of the worry and fear that comes simply with waiting. What if I had the chance to modify his med list, telling them what we take, and ensuring its correctness in his medical record, in real time. What if I could really create a note with his doctor, google docs style - me typing in blue and her in red, the respiratory therapist in orange and the dietician in green and the infectious disease doc in purple, true and total transparency - and what if that enhanced understanding between us, me more clearly understanding her recommendations, and her having a glimpse into my thoughts and feelings, practical and emotional, eliminating errors and misunderstandings, creating an action plan that we both feel confident that we can follow. What if I could look at a calendar online at a time that's convenient for me, selecting who I want to see and when, simultaneously checking my calendar to find a time that works for us and never having to wait on hold while a scheduler tries to solve this for me between the hours of 9-4pm.
What really happened during our appointment last week was captured in the previous post, but if I had it my way, this would be my ideal.
Sunday, June 19, 2016
Tuesday, June 14, 2016
Yesterdays appointment, and problems with the system
Drew had a clinic visit yesterday and it went pretty well! We haven't been to clinic for about 4 months because I didn't want to pull him out of school for an appointment, so with good health, we pushed it out an extra month and went just yesterday. He's been incredibly healthy for the past 18 months, a longer stretch of time without any oral or IV medications than he's ever had which is amazing. His PFTs were low yesterday - not so low that any action needed to be taken but low enough to cause some concern from his doc. But here's the thing - I've seen him do his PFTs before, and while he's still relatively new to the process, he wasn't doing them quite right. I can't put my finger on exactly how it was different, but he wasn't blasting all his breath as hard as he could right off the bat, and I don't think its because he couldn't due to an illness. When he does his breathing treatments at home, he uses a device called an Aerobika that he blows into with long, hard blows that cause a positive pressure in his lungs and opens them up (hes got malacia that makes them extra floppy) and allows him to move mucus. I think he's got the Aerobika technique mixed up with the PFT technique and I'm not sure how to fix it. We are going to come back in two weeks to try again.
Otherwise, the appointment was pretty unremarkable. He's gaining weight like a boss and is happy and healthy and so are we. I'll do a culture this weekend when he's been off of one of his treatments for a few days so we should know more about any new bugs in another week. Fingers crossed we are still just dealing with the beast that is achromobacter. We will also repeat his PFT before we head back to Philly to see if we can get his number back up, and if its still low will have to discuss options to treat or try to figure out what's causing the low number.


Another flaw of the system is appointment scheduling. I need to take Drew back for another appointment in 3 month, and then in 3 months again. I have a preference for the first appointment on a Monday morning, and I also have a preference that we do these appointments at a time that is least disruptive to his life, specifically days off of school. It doesn't matter what anyone else thinks I should do or not do, should deal with or not deal with. This is our life and our preference and we should be allowed to live it according to our own priorities. I digress.
So I called to schedule an appointment for September. In my mind, this should be early enough to schedule an appointment for September 12, a day that he will be off of school. Well there are no appointments available on September 12, only the 19th, and not until later in the morning. So I ask about October, willing to push to the next day off of school so that he's allowed to keep doing what he wants, which is being at school with his buddies and not missing out. Well the schedule for October isn't available yet so I can't schedule for October. I go back to the 19th that they had proposed, however the infectious disease doc that we also see during our appointments isn't available on the 19th so we would have to make a separate appointment to see him. Listen, I don't like to come into a hospital with my kid who is susceptible to dangerous infections in the first place. Now you want me to pull him out of school AND bring him in twice? I'll figure out another solution.
After 12 minutes on the phone I hung up with no appointments and no plan. I can schedule a haircut for my kids from my phone - why can't I log into MyChart and browse through appointment options that work for me? Why does a system that weighs so heavily on patients and families make it so hard to do such simple tasks? What can we do to change this?! And for the record, I don't think these are unreasonable requests. If a motivated, engaged, health-literate adult has this much trouble navigating the system, are we actually maybe causing harm by not addressing these seemingly soft problems?
Otherwise, the appointment was pretty unremarkable. He's gaining weight like a boss and is happy and healthy and so are we. I'll do a culture this weekend when he's been off of one of his treatments for a few days so we should know more about any new bugs in another week. Fingers crossed we are still just dealing with the beast that is achromobacter. We will also repeat his PFT before we head back to Philly to see if we can get his number back up, and if its still low will have to discuss options to treat or try to figure out what's causing the low number.
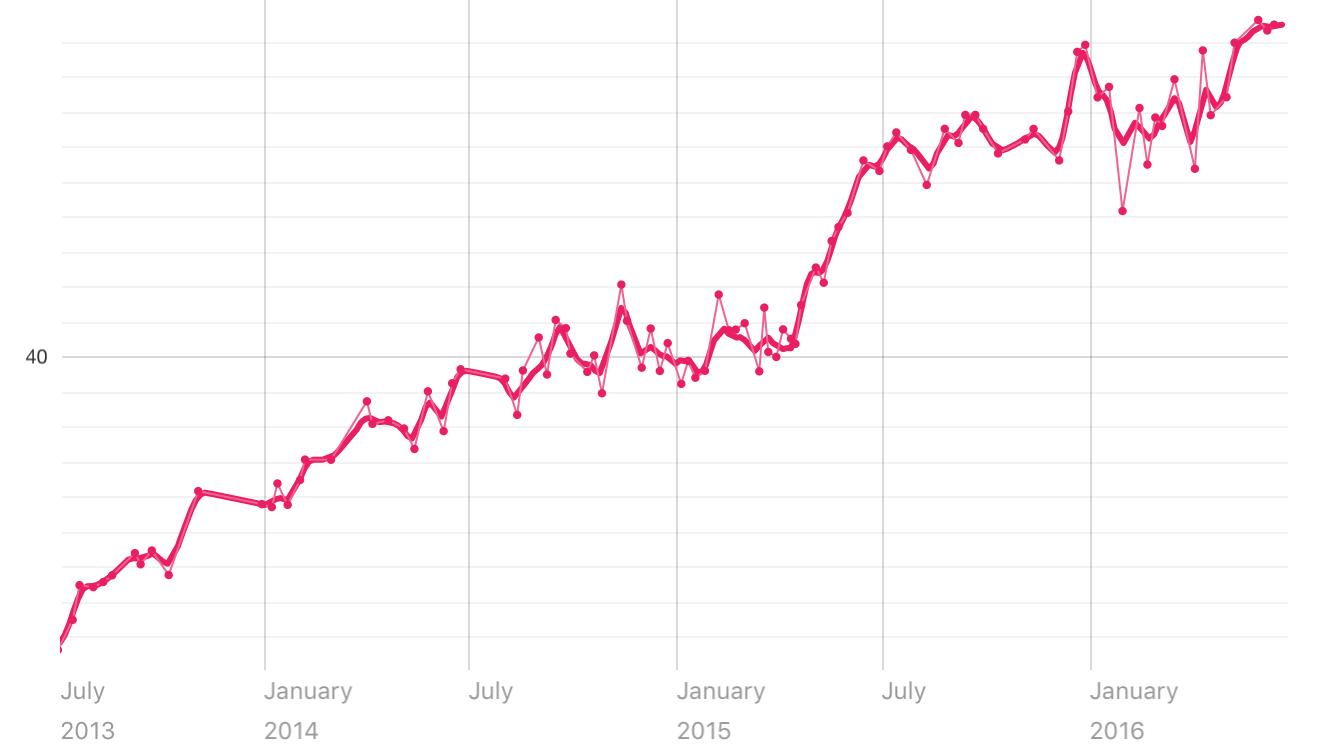
Weight chart from July 2013 to present! BOOM!
The next part of this post is in no way a dig at our hospital or our care team, but rather a general annoyance with the system that I experienced and I've heard many of my peers experience. These are my feelings and opinions and don't reflect that of anyone by myself. And i'm so annoyed that I even stated that.
Per the usual, upon arrival at clinic a nurse or another assistant will come in to take Drew's vitals and then review our med list. And every time, I ask why we are doing it with the response being, "We just want to make sure everything is up to date", though I've yet to see anything change. So we went through the list:
Her: "When was the last time he took Albuterol?"
Me: "4 years ago"
Her: "Atrovent"
Me: "2 years ago"
Her: "Pulmicort"
Me: "6mo ago"
Her: "Azithromycin"
Me: "The liquid or the pill?"
Her: "The liquid"
Me: "3mo"
Her: "The pill?"
Me: "This morning."
Her: "Fluconazole"
Me: "That was just a 3mo treatment"
Her: "So he's off it?"
Me: "Yes"
And on and on and on. We got all the meds hes taking, and "got rid of" the meds he isn't, and we went on with our appointment.
Then before I left, I got my After Visit Summary (AVS), a nice little report of what we discussed during the visit, recommended action steps (make your next appointment, for example), and an updated medication list. Only it's not. Now I don't really care too much whether the med list on my AVS is accurate because I don't use the AVS for much, just a reference or reminder, or to tell my husband what we talked about in clinic. But if it's wrong on my printout, its wrong in my EMR, and the next time I'm asked what med's we are on, we will waste everyone's time by going through this whole process over again. And nothing changes. I've experienced this countless times with homecare nursing, sometimes coming twice a day and having to go through this process, and the list has never, even been right. Before he has gone in for procedures I will review it with someone on the phone the night before, then a nurse in the OR that morning, then again with anesthesia before they take him back and every single time we make the exact same corrections. I think the reason it doesn't change is because only the prescribing physician, the one who put it into the EMR, can take it out, so when you think that the nurse is making the changes they're really just making a note of the changes, flagging them as needing changed, and expecting that the doctor will at some point go in and make the changes. But that doesn't happen, and at no fault of the doc or the nurse or anyone else specifically, except a faulty system. What if something happened to Drew and I wasn't there to tell them what medications he's taking and with what frequency? What if someone less empowered than I used that AVS as a guide for taking their medications? What if there were harmful drug interactions in that list - something new added when the old stuff is never taken away? How might we fix this? The kicker of this image is that is states very clearly that "this list is accurate as of 6/13/16 at 11:59pm". Only it's not.

So I called to schedule an appointment for September. In my mind, this should be early enough to schedule an appointment for September 12, a day that he will be off of school. Well there are no appointments available on September 12, only the 19th, and not until later in the morning. So I ask about October, willing to push to the next day off of school so that he's allowed to keep doing what he wants, which is being at school with his buddies and not missing out. Well the schedule for October isn't available yet so I can't schedule for October. I go back to the 19th that they had proposed, however the infectious disease doc that we also see during our appointments isn't available on the 19th so we would have to make a separate appointment to see him. Listen, I don't like to come into a hospital with my kid who is susceptible to dangerous infections in the first place. Now you want me to pull him out of school AND bring him in twice? I'll figure out another solution.
After 12 minutes on the phone I hung up with no appointments and no plan. I can schedule a haircut for my kids from my phone - why can't I log into MyChart and browse through appointment options that work for me? Why does a system that weighs so heavily on patients and families make it so hard to do such simple tasks? What can we do to change this?! And for the record, I don't think these are unreasonable requests. If a motivated, engaged, health-literate adult has this much trouble navigating the system, are we actually maybe causing harm by not addressing these seemingly soft problems?
Thursday, June 9, 2016
Change is happening now, hop on board
Last week I was invited to an event at the White House through the Office of Science and Technology Policy in a partnership with MedicineX, a conference that I've attended for the past 4 years and have met some of the most amazing people through (you know who you are). The goal of the meeting was to discuss and then start to create ways to engage participants as partners in research, and many good conversations were had. Maybe the best way to explain the problem we were trying to solve is through an example:
Many folks who interact with the healthcare system are often asked to participate in a research project at some point in their medical journey. Whether its for a new cancer treatment or an imagining study for CF patients, we are invited and often times compensated for the time that we spend giving of ourselves to science for the benefit of ourselves and others down the road. Many problems exist with this current plan though. First, it's hard to tell what you're signing up for. There's this thing called "Informed Consent" that usually comes in the form of 8 pages of jargon giving you the risks and benefits of the study where you agree to enter into the research at your own free will. It also sometimes says where and how the data will be used, but I've never really read any of that in anything we've ever done, just simply hearing that we can get $100 for letting them do an MRI to study the difference between an MRI picture of your lungs and a CT scan to better develop ways to capture that data is usually enough for me to say OK. But, sometimes the research that you participate in doesn't recruit enough people to be completed, and then it just disappears as though it never existed in the first place. And sometimes some scientist writes a nice paper about the results and gets credit and money to further their research, and I have to stumble upon it in a journal to learn what they learned and then figure out how or if it applies to me. There's gotta be a better way to respect the contribution that folks make to this research system.
We also discussed recruitment for clinical trials, and how we might help folks to realize the value of the contribution they're making to science and their communities through participation. I'd say to start with, give them their damn data back. Let them know when it will be published. Provide them with updates on the status and findings. And if it fails to recruit, apologize. In other words, be human.
I think what I like most about these meetings is the people that I get to meet. Hearing their wonderful ideas for healthcare improvement and sharing mine, creating partnerships and working together to change things is what matters here. While I know that it's not humanly possible to get all the amazing people into the same room at the same time, some of my favorite people in healthcare that were missing included: Whitney Zatzkin from Flip the Clinic, actually supporting the efforts to turn these ideas into practice; Amy Edgar who stopped admiring the problem of lack of integrated care services for complex kids and actually started a service to meet their needs; Jodi Sperber, user centered Design team lead at Partners Connected Health who gets the value of learning from social networks, and all-around good person; and Beth Toner, an RN and creator of one of my favorite things, The Narrative Playbook. (Look these people up, you won't be disappointed.) While we've all connected through social media, MedicineX has served as a facilitator of many connections beyond that. It puts people in a place to mingle, sparks conversation and ignites ideation. I've seen the conference evolve over the past 4 years, moving from a forum for patients to voice their frustrations and learn about the work going on in the systems around them, to one where we show up without labels, respecting one another for our expertise, whatever that may be. Only a CF mom (or maybe an infectious disease doc) would explain the MedicineX platform and the day at the White House as an effort to create a human biofilm, something so powerful, something impenetrable, unable to be shut down disrupted despite valiant efforts by opposing forces. Change is happening now, for the better, so hop on board.





I've also written about this event at the White House for Eli Lilly's Clinical Trials Blog, LillyPad, where I am now their first ePatient Advisor! Woot!
Many folks who interact with the healthcare system are often asked to participate in a research project at some point in their medical journey. Whether its for a new cancer treatment or an imagining study for CF patients, we are invited and often times compensated for the time that we spend giving of ourselves to science for the benefit of ourselves and others down the road. Many problems exist with this current plan though. First, it's hard to tell what you're signing up for. There's this thing called "Informed Consent" that usually comes in the form of 8 pages of jargon giving you the risks and benefits of the study where you agree to enter into the research at your own free will. It also sometimes says where and how the data will be used, but I've never really read any of that in anything we've ever done, just simply hearing that we can get $100 for letting them do an MRI to study the difference between an MRI picture of your lungs and a CT scan to better develop ways to capture that data is usually enough for me to say OK. But, sometimes the research that you participate in doesn't recruit enough people to be completed, and then it just disappears as though it never existed in the first place. And sometimes some scientist writes a nice paper about the results and gets credit and money to further their research, and I have to stumble upon it in a journal to learn what they learned and then figure out how or if it applies to me. There's gotta be a better way to respect the contribution that folks make to this research system.
We also discussed recruitment for clinical trials, and how we might help folks to realize the value of the contribution they're making to science and their communities through participation. I'd say to start with, give them their damn data back. Let them know when it will be published. Provide them with updates on the status and findings. And if it fails to recruit, apologize. In other words, be human.
I think what I like most about these meetings is the people that I get to meet. Hearing their wonderful ideas for healthcare improvement and sharing mine, creating partnerships and working together to change things is what matters here. While I know that it's not humanly possible to get all the amazing people into the same room at the same time, some of my favorite people in healthcare that were missing included: Whitney Zatzkin from Flip the Clinic, actually supporting the efforts to turn these ideas into practice; Amy Edgar who stopped admiring the problem of lack of integrated care services for complex kids and actually started a service to meet their needs; Jodi Sperber, user centered Design team lead at Partners Connected Health who gets the value of learning from social networks, and all-around good person; and Beth Toner, an RN and creator of one of my favorite things, The Narrative Playbook. (Look these people up, you won't be disappointed.) While we've all connected through social media, MedicineX has served as a facilitator of many connections beyond that. It puts people in a place to mingle, sparks conversation and ignites ideation. I've seen the conference evolve over the past 4 years, moving from a forum for patients to voice their frustrations and learn about the work going on in the systems around them, to one where we show up without labels, respecting one another for our expertise, whatever that may be. Only a CF mom (or maybe an infectious disease doc) would explain the MedicineX platform and the day at the White House as an effort to create a human biofilm, something so powerful, something impenetrable, unable to be shut down disrupted despite valiant efforts by opposing forces. Change is happening now, for the better, so hop on board.





I've also written about this event at the White House for Eli Lilly's Clinical Trials Blog, LillyPad, where I am now their first ePatient Advisor! Woot!
Sunday, June 5, 2016
Our CF Learning Network is launching!
I don't even know where to start with this post, so much has been going on over the past several months that I haven't had a free moment to write. Well, not totally true. Actually I have been writing but its been for our CF Care Model of the Future Newsletter and for the Eli Lilly Blog as I'm now an ePatient advisor working with them! Crazy story of how that all came to be, and specific thoughts on how I (and others) feel about that will be on hold for another post.
You guys, recruitment has started for our CF Learning Network!!! All the work that we've been doing dreaming and designing and planning has gotten us to the point that we are recruiting CF Centers and patients and families to join us to pilot the system that we've dreamed up to test its ability to improve outcomes. Invitations were sent to about 40 CF Centers who were encouraged to identify patients and families to partner together with them to join this work. I'm half ok with the way that it happened - inviting centers to join and identify patients and families to partner with vs. finding the empowered patients and families (of which there are many) and shining a light on them to care centers to join them in their awesome work. We aren't doing it one way or another, but we are capitalizing on the organizational structure of the CF Care Center Network to test out improvement efforts. The awesome patients and families will hopefully join their care teams to learn together and push them to the outer limits of their comfort zone where change happens. We are supporting QI training for teams in this pilot phase so that we can learn a common language, work on projects together, compare results and quickly identify variation and how we can close the gap to get the best care to everyone, personalized, as quickly as possible. I know it sounds abstract, but now that we will soon have a handful of care centers on board and can start to test out some of the ideas that we've dreamed up, I think we will soon be able to talk about it in more concrete terms and start to engage with people at all different levels of interest so that we, as a CF community, can start to work together different to improve outcomes. And I'm not talking about incremental change, I'm talking transformation. I hope (and believe) that within the next 3-5 years, we won't have such dramatic variation in care from center to center but rather best in class care across all CF centers, regardless of where you live and which care center you go to.
A major component of this work will be partnership between patients & parents and the care team, especially those of us who will be working together closely on quality improvement teams. I had a somewhat failed first try at partnership with our care team, and I'm working to learn what successful partnerships have looked like with other learning networks - how patients and parents are working with care team and in what capacity, what's working and what's not from the perspective of both sides. For example, I know a parent partner on one of the IBD teams who works very closely with the care team on their QI efforts as part of the network, runs the patient and family advisory council, but doesn't get paid. She also serves as the go-between for the families and the care team. I had always envisioned more of a partnership, like one big team, rather than two teams (clinicans and families) working together seamlessly. I'm trying to learn what the parents view as valuable and what they wish was different, and also what the care team thinks about that relationship. I have another friend who worked on the patient and family advisiory council with her care team and was asked to leave when she expressed opposition to some of their work. She's a powerhouse in healthcare improvement, respected by many inside of and outside of the CF world, and can't work with her care team because they wanted a cheerleader, someone to talk about the great work they're doing, and when she challenged them to think bigger they called her negative and asked her to leave. Another parent partnered her non-profit organization that she started, completely independent of any care center, with the National Pediatric Cardiology Quality Improvement Collaborative, the learning network for babies with HLHS, and they have a fabulous relationship. It seems that there will be a variety of ways for folks to partner in this work - some with the care team leading, some with patients leading, some with true partnership and perhaps even some independent work, and I'm really trying to crack that nut of engagement opportunities that exist for all players in our learning health system. Maybe I'll attempt to draw it out on here once I figure it out. Or at least share the ideas I come up with.
Drew has been well. Like really well. Like I haven't talked about him on the blog in 18months because hes not been since in 18months and I don't wanna jinx it. He didn't miss any school this year and hasn't had a PICC since March of 2015 and thats amazing for any number of reasons. He had an annual pediatrician appointment last week and he gained 8lbs this year, compared to the 2lbs he had gained between 2014-2015. Things have just been well, so i'll leave it at that.
We're deep into summering right now - staying up a little later than we normally allow, spending endless hours at the pool, taking lots of mini trips and embracing the lack of a schedule. I'm sure that by mid July I'll be longing for that schedule again, but right now it is still such a welcomed break from all that the school year gave us. We're heading to St. Louis to meet some friends in a few weeks, and then back to PA for the last week of June and first week of July before a family trip to South Carolina at the end of July. I'm not sure how I'll do all the work I committed to prior to the official dawn of summer, but I'm sure I'll figure it out. Up next, that time I went to the White House, episode 3. Stay tuned!
You guys, recruitment has started for our CF Learning Network!!! All the work that we've been doing dreaming and designing and planning has gotten us to the point that we are recruiting CF Centers and patients and families to join us to pilot the system that we've dreamed up to test its ability to improve outcomes. Invitations were sent to about 40 CF Centers who were encouraged to identify patients and families to partner together with them to join this work. I'm half ok with the way that it happened - inviting centers to join and identify patients and families to partner with vs. finding the empowered patients and families (of which there are many) and shining a light on them to care centers to join them in their awesome work. We aren't doing it one way or another, but we are capitalizing on the organizational structure of the CF Care Center Network to test out improvement efforts. The awesome patients and families will hopefully join their care teams to learn together and push them to the outer limits of their comfort zone where change happens. We are supporting QI training for teams in this pilot phase so that we can learn a common language, work on projects together, compare results and quickly identify variation and how we can close the gap to get the best care to everyone, personalized, as quickly as possible. I know it sounds abstract, but now that we will soon have a handful of care centers on board and can start to test out some of the ideas that we've dreamed up, I think we will soon be able to talk about it in more concrete terms and start to engage with people at all different levels of interest so that we, as a CF community, can start to work together different to improve outcomes. And I'm not talking about incremental change, I'm talking transformation. I hope (and believe) that within the next 3-5 years, we won't have such dramatic variation in care from center to center but rather best in class care across all CF centers, regardless of where you live and which care center you go to.
A major component of this work will be partnership between patients & parents and the care team, especially those of us who will be working together closely on quality improvement teams. I had a somewhat failed first try at partnership with our care team, and I'm working to learn what successful partnerships have looked like with other learning networks - how patients and parents are working with care team and in what capacity, what's working and what's not from the perspective of both sides. For example, I know a parent partner on one of the IBD teams who works very closely with the care team on their QI efforts as part of the network, runs the patient and family advisory council, but doesn't get paid. She also serves as the go-between for the families and the care team. I had always envisioned more of a partnership, like one big team, rather than two teams (clinicans and families) working together seamlessly. I'm trying to learn what the parents view as valuable and what they wish was different, and also what the care team thinks about that relationship. I have another friend who worked on the patient and family advisiory council with her care team and was asked to leave when she expressed opposition to some of their work. She's a powerhouse in healthcare improvement, respected by many inside of and outside of the CF world, and can't work with her care team because they wanted a cheerleader, someone to talk about the great work they're doing, and when she challenged them to think bigger they called her negative and asked her to leave. Another parent partnered her non-profit organization that she started, completely independent of any care center, with the National Pediatric Cardiology Quality Improvement Collaborative, the learning network for babies with HLHS, and they have a fabulous relationship. It seems that there will be a variety of ways for folks to partner in this work - some with the care team leading, some with patients leading, some with true partnership and perhaps even some independent work, and I'm really trying to crack that nut of engagement opportunities that exist for all players in our learning health system. Maybe I'll attempt to draw it out on here once I figure it out. Or at least share the ideas I come up with.
Drew has been well. Like really well. Like I haven't talked about him on the blog in 18months because hes not been since in 18months and I don't wanna jinx it. He didn't miss any school this year and hasn't had a PICC since March of 2015 and thats amazing for any number of reasons. He had an annual pediatrician appointment last week and he gained 8lbs this year, compared to the 2lbs he had gained between 2014-2015. Things have just been well, so i'll leave it at that.
We're deep into summering right now - staying up a little later than we normally allow, spending endless hours at the pool, taking lots of mini trips and embracing the lack of a schedule. I'm sure that by mid July I'll be longing for that schedule again, but right now it is still such a welcomed break from all that the school year gave us. We're heading to St. Louis to meet some friends in a few weeks, and then back to PA for the last week of June and first week of July before a family trip to South Carolina at the end of July. I'm not sure how I'll do all the work I committed to prior to the official dawn of summer, but I'm sure I'll figure it out. Up next, that time I went to the White House, episode 3. Stay tuned!